Vaccination and HPV screening
The target population of women born between 1994–1999 and residents in the greater Stockholm County was found to encompass 89,547 women. All received personal invitations. One hundred and fifty-seven women (0.18%) declined participation, leaving a target group of 89,390 women (Fig. 1).
There were 26,105 women (29.2% of the total target population) who consented, were vaccinated, and offered HPV testing (either by cervical sampling by midwives or as self-sampling) between 2021-05-03 and 2022-12-31 (Table 1). For the present paper, we included all HPV tests submitted and analysed by February 28th, 2023 (2 months after the last vaccination date, allowing for reasonable delays in taking the sample, posting and analysing it). By February 28th, 2023, 22,557/26,105 women (86.4%) had an HPV test on file taken at or after the vaccination (Table 1). Among these, most HPV tests (13,460/22,557, 59.7%) were based on self-sampling. There were 8,667 samples (38.4%) midwife-taken and a few clinical samples (430 samples, (1.91%)). The exact reason for taking these clinical samples is not known, but it could be, for instance, that a woman had a scheduled appointment with a private gynecologist and did not take the self-sample because of the gynecologist-taken sample.
Table 1
Type-specific HPV prevalences at baseline enrollment in the population-based trial of concomitant HPV vaccination and HPV screening.
| Birth year | Number | Prior | Number of | Number of | HPV 16 | HPV18 | HPV45 | HPV 33/58 | HPV 31 | HPV 52 | Other HPV* | HPV neg | Invalid |
| of women in population | Vaccination offered | those women vaccinated | those women HPV tested |
| 1994 | 18436 | Catch-up | 5687 | 4941 | 122 | 26 | 118 | 191 | 106 | 117 | 611 | 3609 | 41 |
| % | | 30.85 | 86.88 | 2.47 | 0.53 | 2.39 | 3.87 | 2.15 | 2.37 | 12.37 | 73.04 | 0.83 |
| 1995 | 16761 | Catch-up | 5120 | 4428 | 98 | 24 | 148 | 170 | 98 | 126 | 548 | 3175 | 41 |
| % | | 30.55 | 86.48 | 2.21 | 0.54 | 3.34 | 3.84 | 2.21 | 2.85 | 12.38 | 71.7 | 0.93 |
| 1996 | 15619 | Catch-up | 4788 | 4176 | 72 | 18 | 118 | 138 | 74 | 131 | 582 | 3012 | 31 |
| % | | 30.65 | 87.22 | 1.72 | 0.43 | 2.83 | 3.3 | 1.77 | 3.14 | 13.94 | 72.13 | 0.74 |
| 1997 | 13971 | Catch-up | 4108 | 3465 | 73 | 26 | 93 | 143 | 65 | 97 | 536 | 2405 | 27 |
| % | | 29.4 | 84.35 | 2.11 | 0.75 | 2.68 | 4.13 | 1.88 | 2.8 | 15.47 | 69.41 | 0.78 |
| 1998 | 12802 | Catch-up | 4020 | 3419 | 73 | 16 | 67 | 125 | 41 | 77 | 695 | 2303 | 22 |
| % | | 31.4 | 85.05 | 2.14 | 0.47 | 1.96 | 3.66 | 1.2 | 2.25 | 20.33 | 67.36 | 0.64 |
| 1999 | 11801 | School-based | 2382 | 2128 | 15 | 1 | 34 | 92 | 22 | 81 | 285 | 1584 | 14 |
| % | | 20.18 | 89.34 | 0.7 | 0.05 | 1.6 | 4.32 | 1.03 | 3.81 | 13.39 | 74.44 | 0.66 |
| TOTAL | 89390 | 86 | 26105 | 22557 | 453 | 111 | 578 | 859 | 406 | 629 | 3257 | 16088 | 176 |
| % | | 29.2 | 86.41 | 2.01 | 0.49 | 2.56 | 3.81 | 1.8 | 2.79 | 14.44 | 71.32 | 0.78 |
| *Other HPV correspond to the results obtained as a pool from the Cobas platform (HPV types 31/33/35/39/45/51/52/56/58/59/66/68) that could not be retested in the BD platform for extended genotyping as well as those tested with the BD platform that are classified as low oncogenic types (HPV35/39/51/56/59/66/68) |
In 2022, the organized screening program switched from partial (HPV16/18/Other) to extended genotyping for routine testing of HPV samples. Therefore, samples positive for “other HPV” had to be re-analysed with extended genotyping. From 14,377 samples analysed only with partial genotyping, 4,146 were positive for “other HPV” and these were re-analysed with extended genotyping. For 3,129/4,146 such specimens, results were obtained for extended genotyping, but 1,017 samples could not be re-analyzed (sample not biobanked or low quantity of sample material left).
About 28% of samples were HPV-positive (Table 1). However, most of the HPV positivity was for the low oncogenicity HPV types that are not targeted by the nonavalent HPV vaccine. The three most oncogenic HPV types - HPV 16, HPV 18 and HPV 45 - were present in 2.0%, 0.5%, and 2.6% of the samples, respectively (Table 1). The proportion of invalid samples was 0.8% (Table 1).
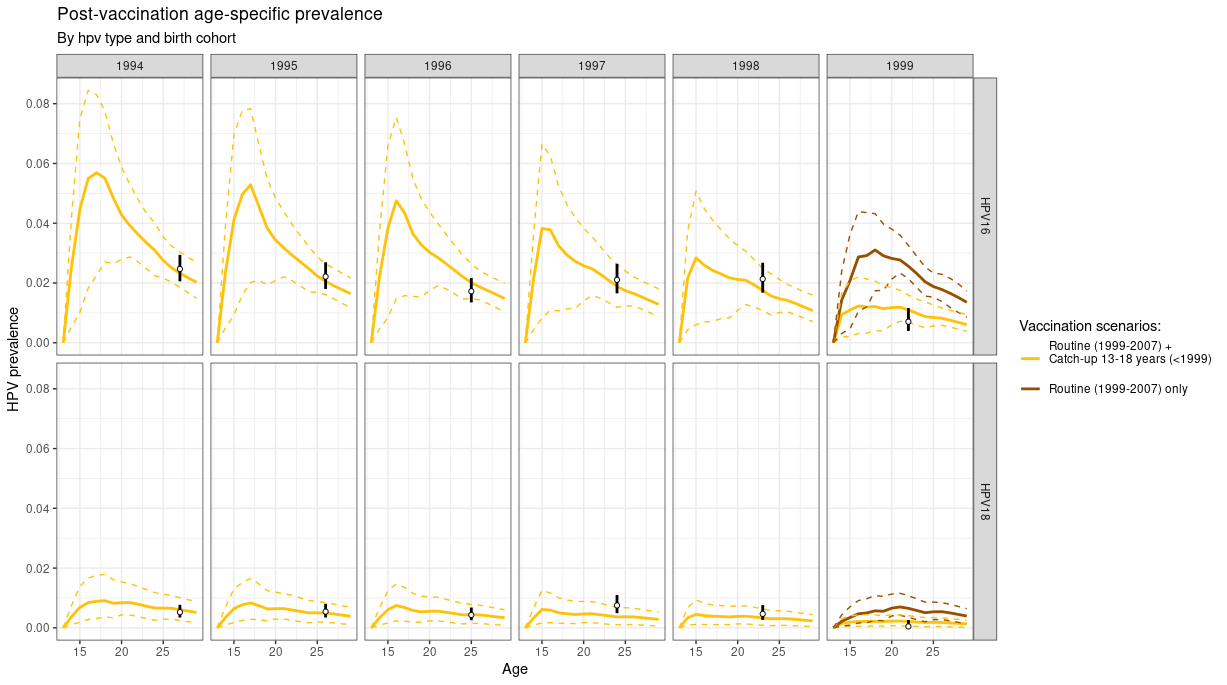
The prevalence of the major HPV types targeted by the first-generation vaccine (HPV 16 and 18) was low among the women who had been offered organised, school-based HPV vaccination that achieved high coverage (born 1999). 6 An effect of vaccination on HPV prevalences was also seen in women offered catch-up vaccination (born 1994–1998, moderate coverage) (Table 1). The prevalences of HPV types not targeted by the vaccine (and not having known cross-protection) seemed stable among cohorts that had no organised vaccination.
Predicted effects of the trial
The projected incidence over time of HPV 16 (upper panels) and HPV 18 (lower panels) as a function of the different attendance rates in the trial are shown in Fig. 2, starting with the observed 30% attendance rate in Stockholm County as of 2022-12-31 (present study) and with predicted gains if attendance can be increased (with time), or if enrolment is more successful in other counties.
As expected, the largest gains in reduction of HPV 16/18 incidence are found in the birth cohorts targeted by the trial who had previously been targeted only by catch-up vaccination (born 1994–1998). For example, this age group had an HPV 16 incidence of 9.1 (per 100 women-year) in 2020 which, with the trial attendance reported in this paper (30%), will decline to 3.6 in 2024, as compared to the decline expected if no trial had been launched (from 9.1 to 5.6). As shown in Fig. 2 insets, increasing the trial coverage will further reduce incidence. There were negligible gains in the birth cohorts that did not have any organised vaccination before and were not targeted by the trial (born 1989–1993). For example, the HPV 16 incidence decreased in this age group from 11.2 (per 100 women-year) in 2020 to 1.2 in 2028 and further to 0.5 in 2035 – but with the same decline seen regardless of the current trial. There are some gains in the age group targeted by high coverage school-based vaccination (born 1999–2003) where only the girls born 1999 are targeted by the trial (as comparison group). The HPV 16 incidence is 4.2 (per 100 women-year) in 2020 and this will decline to 2.3 in 2024 (assuming a 30% trial attendance), as compared to the 2.7 incidence predicted in 2024 if no trial had been launched). The timing between the enrolment test and the trial follow-up test (3 years) is displayed as a shaded area. As can be seen, the full protection of the trial is not realised immediately as it takes some time before secondary protection (herd immunity) develops. Similar patterns are predicted for HPV 18 (Fig. 2).
{kind=link}