In the present study, we demonstrate that positive ER or PR status measured by cytosol-based methods, IHC, and GEX analysis, is predictive of tamoxifen benefit for premenopausal patients with invasive breast cancer. The methods were equally good at predicting benefit of tamoxifen supporting that the methods can be interchangeable. Tamoxifen is still widely used as an adjuvant therapy in premenopausal women and the present finding that mRNA levels of hormone receptors carry tamoxifen predictive information is thus clinically relevant. In the present trial, two years of tamoxifen was evaluated in contrast to today´s recommendation of five or more years. However, prediction of the effect of two years of tamoxifen is today important for patients aiming to get pregnant after a breast cancer diagnosis, since these patients will be recommended to interrupt adjuvant endocrine therapy after two years. Additionally, side effects prevent some patients from completing the specified treatment course of at least five years (23).
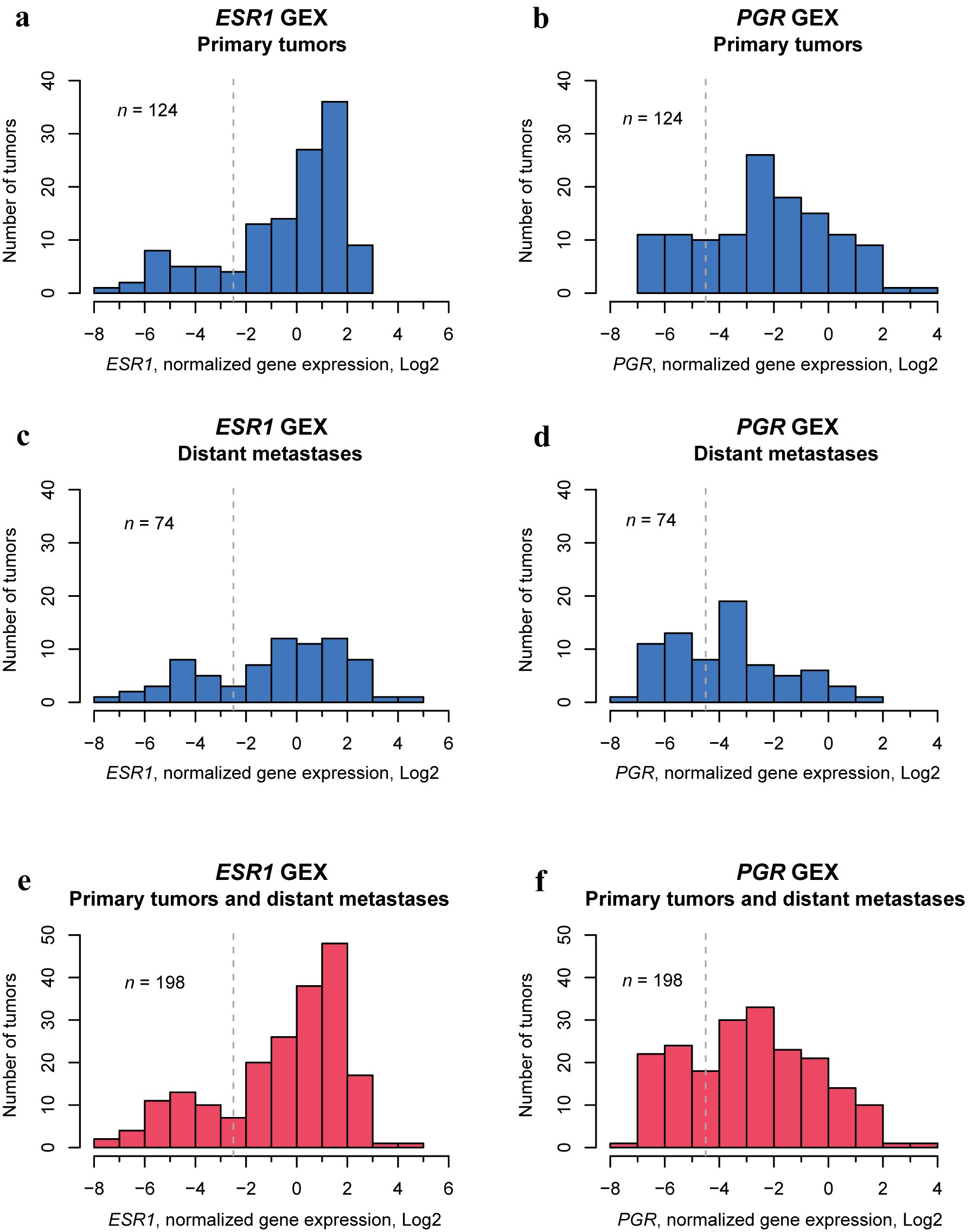
mRNA levels of ESR1 and PGR had bimodal distributions, suggesting that there may be a clear discrimination between patients with hormone receptor-positive and -negative tumors at the mRNA level. To our knowledge, no previous publication has demonstrated this bimodal distribution of mRNA levels of the ESR1 and PGR genes. Furthermore, mRNA levels strongly correlated to protein expression analyzed by cytosol-based methods and IHC, indicating that mRNA levels are a good surrogate marker for protein expression when analyzing hormone receptors.
In line with the findings of this study, where the concordances between all three methods were 84% (ER) and 85% (PR), previous studies have reported concordance around 87% (ER) and 86% (PR) between cytosol-based methods and IHC for assessment of protein expression, and around 92% (ER) and 89% (PR) between protein expression by IHC and GEX analysis (24, 25, 26, 27). The slightly lower concordance reported in the present study may be due to the comparison of three methods instead of two, and the relatively small number of exclusively premenopausal patients included. To our knowledge, no previous publication has compared all three methods.
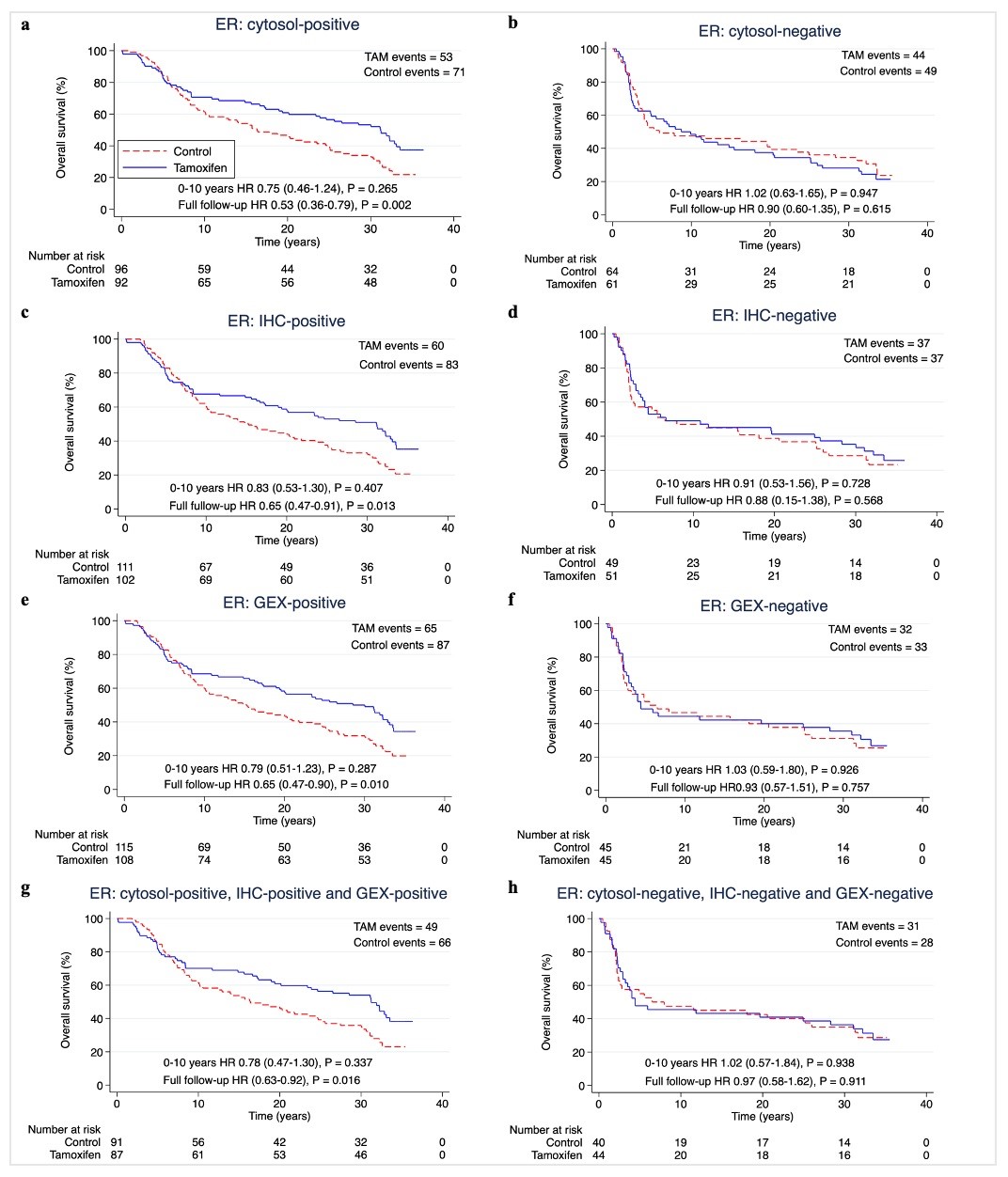
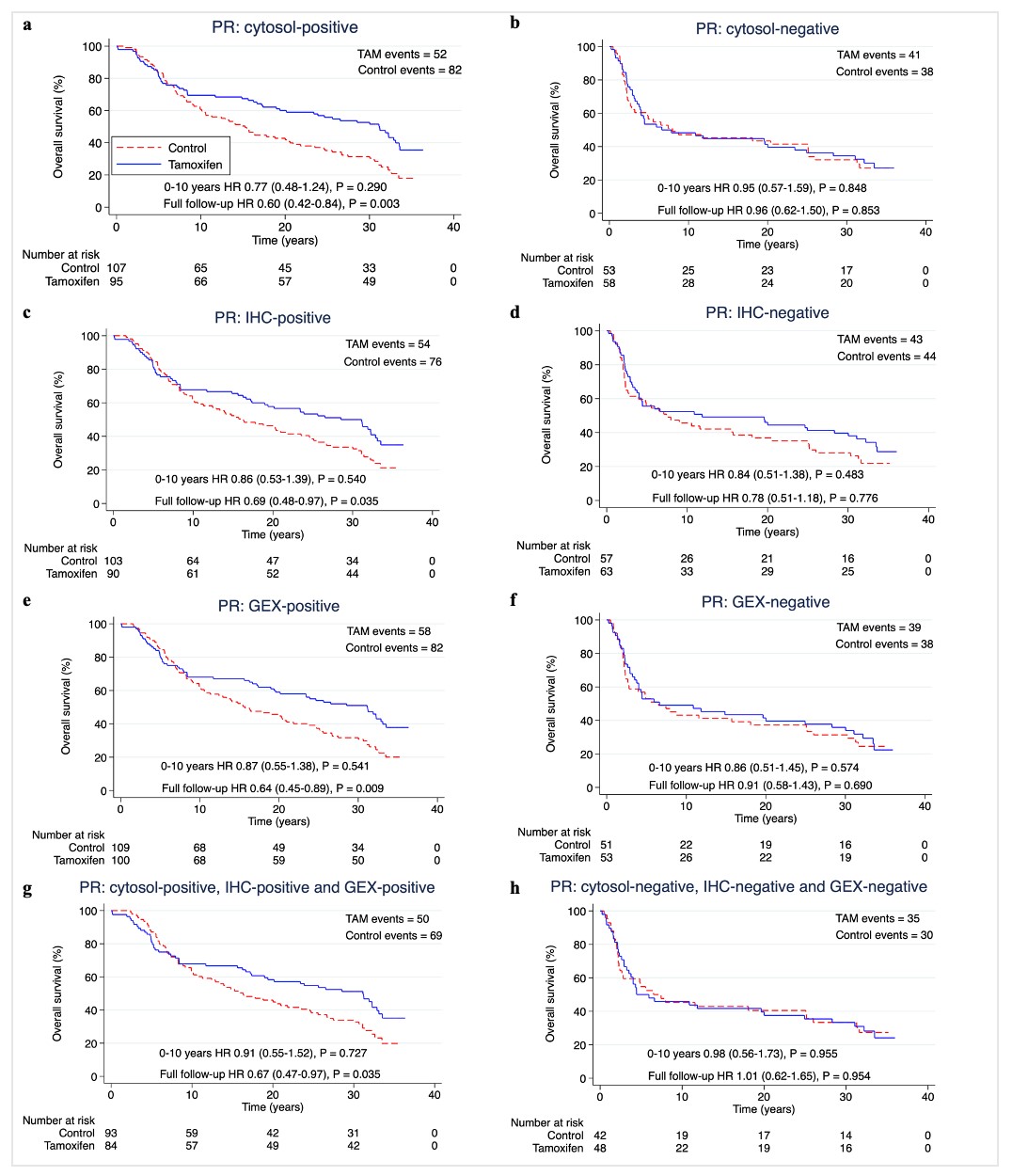
Patients receiving tamoxifen had longer RFi if their tumor was ER + or PR + regardless of the applied method for receptor determination. In patients with tumors that were ER + or PR + by either method, the HRs for tamoxifen were similar, indicating that the methods are equally good at identifying patients who benefit from tamoxifen. Combining all three methods to consider “triple-positive” tumors did not seem to improve the predictive performance, as “triple-positive” tumors had equal benefit of tamoxifen as “single-positives”. These results suggest that cytosol-based methods or IHC assessment for protein expression, and GEX analysis of hormone receptors perform equally well and are interchangeable as predictive tools. A larger cohort study would be needed to determine this. Finally, a larger study could address patients with discordant results that in this study, due to the small number (ER: 51/313; PR 46/313), were not further tested statistically.
It is well known that both cytosol-based methods and IHC for determining hormone receptor status can be used for prediction of tamoxifen benefit (3, 28). Interestingly, this study found that GEX of ESR1 and PGR could be used as well. In a study by Kim et al. (5) patients were randomized to tamoxifen or placebo irrespectively of menopausal status and distant RFi at ten years were compared according to mRNA levels of ESR1 and PGR. The authors found that high ESR1 mRNA levels were associated with tamoxifen benefit, while GEX of PGR lacks predictive function (5). Throughout this study, also positive PR status determined by any method seemed to be predictive of tamoxifen benefit. This result may differ from the EBCTCG report that stated that, given the ER status, PR status does not give any additional predictive information (3). In the present study, including premenopausal patients only, most PR + patients were ER+, which might be a reason for the tamoxifen response observed in the PR + subgroups. Nevertheless, several studies have demonstrated a predictive value for PR independently of ER status (29, 30, 31).
In the analysis of OS at ten years, the evidence for tamoxifen benefit was lower compared to the analysis of RFi. Although, HRs for patients positive for ER and PR by any method were lower in the tamoxifen arm than the control arm. With around three decades of follow-up, tamoxifen improved OS, as previously reported by Ekholm et al. (11) for patients with ER + tumors in this trial. They also found a trend of decreased cumulative mortality (including death of all causes) for ER + patients receiving tamoxifen for the same follow-up time. In a study by Khoshnoud et al. (24), IHC, and cytosol-based methods for the determination of ER status in postmenopausal women were compared regarding the ability to predict benefit of tamoxifen. Patients were randomized to two years of adjuvant tamoxifen or no systemic treatment (24). The authors found that both IHC and cytosol-based methods could identify patients that had benefit from tamoxifen in terms of recurrence-free survival, but also had lower evidence against the null hypothesis of no difference in OS. The authors concluded that IHC and cytosol-based methods were interchangeable for the prediction of tamoxifen benefit, which supports the results of the present study (24).
For RFi, ER status by GEX analysis and PR-status by cytosol-based methods had the lowest interaction P-values with tamoxifen treatment. In the study by Kim et. al (5), the authors also found a tamoxifen treatment interaction with high mRNA levels of ESR1 in relation to distant RFi. A larger study population is needed for more statistical power and reliability in interaction analyses.
The strengths of this study are its randomized design, long follow-up, and that most of the patients only received tamoxifen as systemic treatment, or no systemic treatment. The latter provides an opportunity to study the effects of tamoxifen independent of other systemic treatments. Another strength is that we provide a proof-of-concept analysis for the proposed data-driven cutoff strategy for GEX of ESR1 and PGR in an independent cohort of metastatic breast cancer. Observing that the GEX of both genes is bimodally distributed in both primary tumors and distant metastases – with similar cutoff – suggests that this method is transferrable to other cohorts and tumor stages. Limitations include the number of patients. The selection of 313 patients with data available for all three measuring methods out of the 564 patients that were originally randomized could potentially lead to bias. However, patients and tumor characteristics of the included and excluded subgroups showed no noticeable differences between the two groups (Table 1). A limitation in transferability includes the use of the cut-off > 10% for IHC, which differs from the cutoffs often used globally (4). Furthermore, today patients are given at least five years of tamoxifen instead of two, and receive additional treatments (7, 32). However, five to ten years of treatment can be problematic for premenopausal patients wishing to become pregnant, making studies of shorter treatment regimens of tamoxifen interesting. Importantly, the recently presented trial by Partridge et al. (33) concluded that interruption of endocrine treatment after 18–30 months, was not associated with an increased risk of recurrence compared to an external control cohort which did not interrupt treatment. Furthermore, when the SBII:2pre trial was conducted, the overall prognosis for premenopausal breast cancer patients was worse than today (34). As an example, HER2-positive patients included in the study did not receive trastuzumab, which would have affected their prognosis.
The finding that GEX of ESR1 and PGR can be used to predicting tamoxifen benefit is clinically useful since GEX analysis already is routinely performed in patient subgroups with early breast cancer. Importantly, several gene assays used for this purpose, including Oncotype DX® and Prosigna®, include data on ESR1 and PGR expression (7, 8, 9, 20, 35). In the future, ESR1 and PGR data from these patients could potentially be used for hormone receptor determination as an alternative to IHC.
{kind=link}
{kind=link}
{kind=link}