Date sources and study population
This is a observational cohort study performed by using participants’ date from the DRYAD public database (https://datadryad.org). Initially, the records of 20,944 participants who attended a comprehensive medical examination program at Murakami Memorial Hospital between 2004 and 2015 were extracted by Okamura T et.al.[15, 16] The details of the medical health check-up programme were described previously.[15, 17]Individuals were excluded at baseline for the following reasons: 1) no available records for abdominal ultrasonography and important variables including age, sex, BMI, waist circumference (WC), blood pressure, or fasting plasma glucose (FPG), triglycerides (TG), and glycated hemoglobin (HbA1c) levels; 2) other known chronic liver diseases, such as liver cirrhosis (history or findings on ultrasound), viral hepatitis (defined by serum positive serological markers for HBV or HCV), or alcoholic fatty liver disease (mean alcohol consumption at least 60 g for males and 40 g for females per day); 3) use of any medication; or 4) diagnosed with diabetes or impaired fasting glucose (IFG) at baseline. To avoid reverse association, individuals with a follow-up period < 1 yearwere excluded, Moreover, participants with an undefined diabetes status at the follow-up visit were also excluded. Some participants met more than one exclusion criterion. Ultimately, 14,482 subjects were selected for further analysis in the present study (Figure 1).
This study conformed to the Declaration of Helsinki.Given that our date were obtained from the public database, no prior ethical approval was required. The requirement for informed consent was also waived as the data were anonymous.
Data acquisition
As described in the previous study,[15] at each visit to the health check center, the participants’ demographic data, including age, sex, smoking status, drinking status, exercise habits and medication history, were acquired from a standardized questionnaire by the same trained team of interviewers. Smoking status was categorized as non, ex-, or current smoker.[18] Individuals who performed any type of physical activity at least once a week on a regular basis were considered regular exercisers.[19] Average alcohol consumption per week was calculated by asking the frequency and amount of alcoholic beverage during the prior month. Grade of alcohol consumption was defined as follows: no or minimal (< 40 g/wk); light (40 - 140 g/wk); moderate (>140 g/wk).[20] Physical parameters, including height, weight, waist circumference, and blood pressure, were measured by trained investigators under standardized conditions according to a standard protocol. BMI was calculated as weight in kilograms divided by height in meters squared, and the result is expressed in units of kg/m2.
Venous blood specimens drawn from the antecubital vein were obtained after an overnight fast of at least 8 h. Laboratory analyses, including TGs, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), gamma glutamyltransferase (GGT), HbA1c, FPG, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) levels, were carried out in accordance with relevant guidelines and regulations using a Modular Analytics system (Hitachi High-Technologies Corp., Ltd., Tokyo, Japan), which is widely applied for biochemical analysis in Japan.
Abdominal ultrasonographic examinations were performed by trained sonographers using an Aloka SSD-650CL ultrasound machine (Aloka Co., Ltd., Tokyo, Japan) at baseline, and all ultrasonographic images were stored as photocopies.[18] Fatty liver was diagnosed by gastroenterologists according to the following four known criteria: hepatorenal echo contrast, liver brightness, gradual attenuation of far-field, and vascular blurring.[21] The clinicianswere all blinded to the clinical data of the participants.
Endpoint and definitions
The endpoint was the occurrence of incident diabetes during the follow-up period. According to the diagnostic criteria of the American Diabetes Association,[22] diabetes was defined as FPG level ≥ 7.00 mmol/L and/or HbA1c ≥ 6.5% and/or self-reported diabetes that was previously diagnosed by a physician and/or current use of anti-hyperglycemic agents.
NAFLD was defined as the presence of fatty liver in the absence of excessive alcohol consumption. There is no standard definition of lean NAFLD; however, numerous studies recommended a cut-off point of BMI 23 kg/m2 for Asian populations,[23-25] and the following four groups were assessed: lean without NAFLD, lean with NAFLD, overweight/obese without NAFLD, and overweight/obese with NAFLD. For further NAFLD categorization, a representativenoninvasive score was used to assess the severity of fibrosis. BAAT scores consist of the sum of the following categorical variables: BMI (≥ 28 kg/m2 = 1), age (≥ 50 years=1), ALT [≥ 2UNL (male ≥ 60 IU/L; female ≥ 40 IU/L) =1], and triglycerides (≥ 1.7 mmol/L= 1). Patients with NAFLD were further categorized into two groups: low (BAAT < 2) and high (BAAT ≥2) probability of advanced fibrosis.[26]
Visceral-fat obesity was defined as a waist circumference≥90 cm in males or ≥ 80 cm in females.[27]
Statistical analysis
Categorical variables are presented as counts (percentages), and continuous data are expressed as means (standard deviations, SD). The characteristics of the study participants at baseline are summarized in Table 1, and significant differences among the four groups were analyzed by one-way analysis of variance (ANOVA) followed by the LSD post hoc test and Chi-square test for continuous variables and categorical variables, respectively.
Cox proportional hazards regression analyses were performed to calculate hazard ratios (HRs) with 95% confidence intervals (CIs) for incident diabetes according to different phenotypes, with patients with a lean status and without NAFLD defined as the reference group. We used three models with progressive adjustments: model 1 was adjusted for age and sex; model 2 was further adjusted for smoking status (non-, ex-, or current), grade of alcohol consumption (no/minimal, light, or moderate), and regular exerciser; model 3 was further adjusted forvariables associated with metabolic syndrome,including visceral-fat obesity (presence or absence), blood pressure (SBP and DBP), triglycerides, total cholesterol, HDL-c, and HbA1c. Potential confounders in multivariable models were selected based on their associations with the outcome or a change in effect estimate of more than 10%.
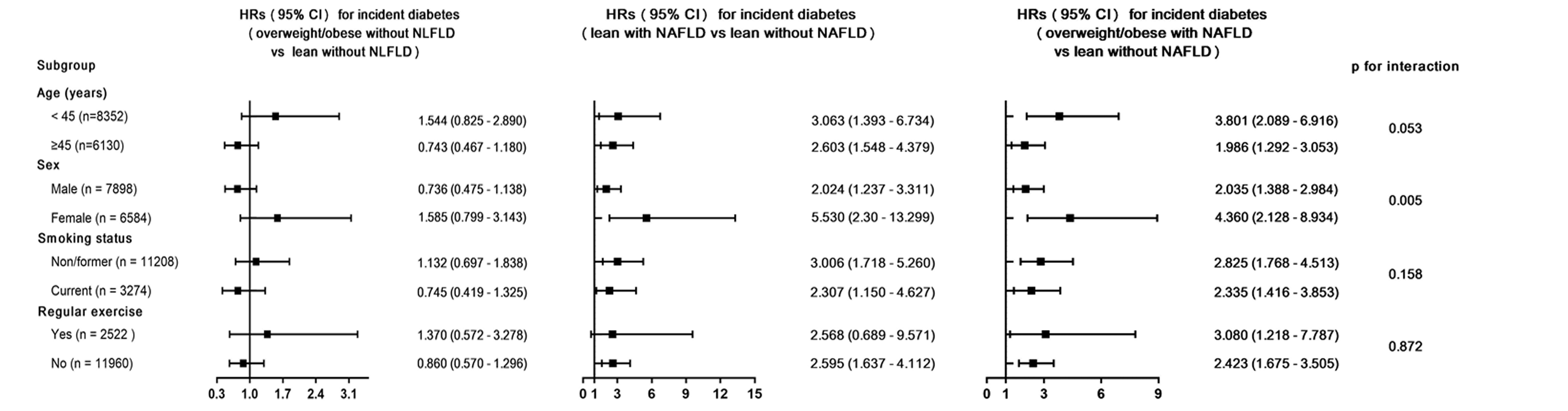
Stratified analyses were conducted in various subgroups, and their interactions were also tested. Each stratification adjusted for all the factors (age, sex, smoking status, grade of alcohol consumption, regular exerciser, visceral-fat obesity, blood pressure, triglycerides, total cholesterol, HDL-c, and HbA1c), except for the stratification factor itself. Moreover, we evaluated the effect of the severity of NAFLD on incident diabetes using Cox proportional hazards modeling, in which models were not adjusted for age or triglycerides, as these factors were included in the calculation of BAAT scores. Statistical analyses were conducted in IBM Statistical Package for the Social Sciences (SPSS) 21 (version 21.0, Armonk, NY). A two-tailed p-value < 0.05 was considered statistically significant.
{kind=link}