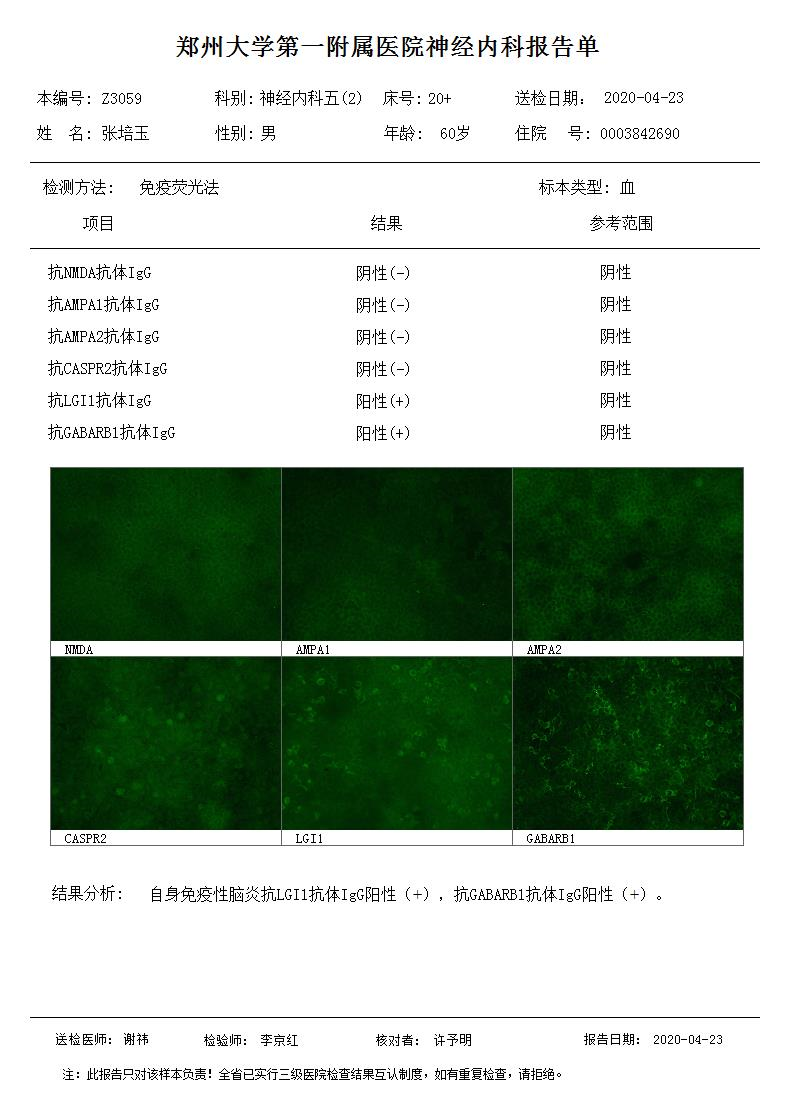
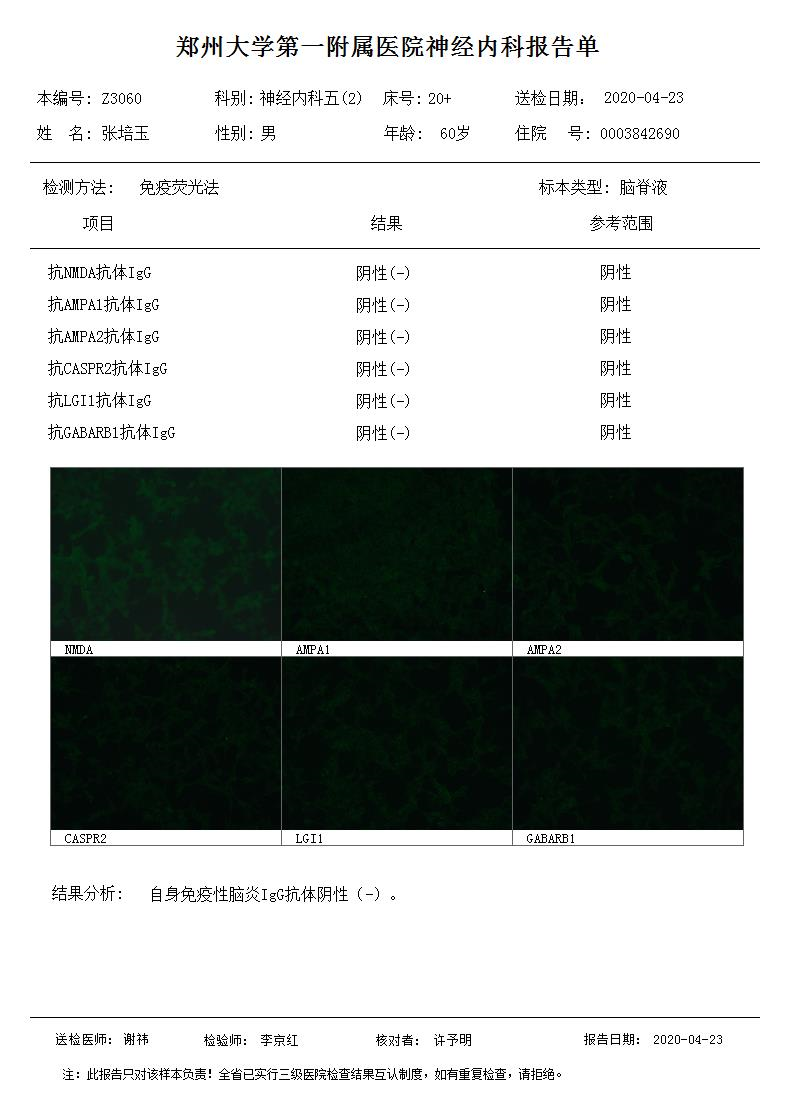
Co-existence of serum anti-LGI1 and anti-GABABR in AE patient has not been previously reported. The 60-year-old patient, with subacute onset, mainly manifested cognitive decline, behavioral abnormality and hyponatremia. The serum anti-LGI1 and anti-GABABR were double positive, and EEG indicated moderate diffusion abnormality. According to the patients' symptoms, AE auto-antibody spectrum test and EEG results, the patient was diagnosed as AE with double auto-antibody positive, ie, anti-LGI1 and anti-GABABR. The patient responded well to glucocorticoid treatment, and we will continue to follow up the prognosis.
Anti-LGI1 encephalitis, which is mostly found in elderly men with subacute onset, is related to hyponatremia caused by syndrome of inappropriate antidiuretic hormone secretion. Most patients demonstrated cognitive impairment, and about 90% of them have behavioral and/or personality changes. Frequent seizures, especially focal seizure, are seen in the majority of patients, while generalized tonic clonic seizures are not very common. Most patients have no related tumors, only about 10% had thymoma, while other tumors were rare. Up to 75% of cases have normal CSF routine analysis. EEG can show mild diffuse slow wave, and about half may have swelled medial temporal lobe with high T2/flair signal. The good news is the relatively low recurrence rate[3-4]. Anti-GABABR encephalitis mostly presents limbic encephalitis symptoms, with temporal lobe epilepsy as the core symptomatology, and most of them are accompanied by cognitive function decline, personality change and mental behavior abnormality. About 50% of patients have small cell lung cancer or neuroendocrine tumor. It is suggested that anti-GABABR encephalitis should further take chest CT or PET examination[5].
The overlying of neuronal auto-antibodies may cause the superposition of clinical syndrome, but not a simple complete superposition, which needs to be analyzed according to the specific antibody type and clinical manifestation. According to Professor Guan Hongzhi's newly published review, it is necessary to distinguish whether the antibodies in patients belong to pathogenic markers or concomitant antibodies[6]. The main manifestations of this case are psychobehavioral abnormality and hyponatremia, more similar to clinical manifestations of anti-LGI1 AE.
The co-existence of multiple auto-antibody is rare(summarized in Table 2). Ren Haitao reported 531 cases of AE with auto-antibodies, and only 10 cases detected multiple anti-neuronal antibodies, among whom 5 cases were anti-GABABR/anti-Hu(+), 1 anti-NMDAR/APQ-4(+), 1 anti-LGI1/anti-CASPR2(+), 1 anti-LGI1/anti-Yo(+), 1 anti-AMPAR/anti-CV2(+) and 1 anti-AMPAR/anti-Hu(+)[6]. In the 20 anti-GABABR AE cases reported by Hoftberger, 7 detected multiple auto-antibodies, among whom 3 cases with anti-Sox1, 1 with anti-Ri, 1 with anti-amphiphysin, 1 with anti-GAD65 and 1 with anti-NMDAR[7]. Liu XY recently reported one case characterized by double positive of anti-LGI1 and anti-NMDAR[8]. Boronat reported a case of anti-GABABR combined with anti-GAD65, menifestating cerebellar ataxia and thymoid carcinoid[9]. Qi Hengchang reported two cases of AE with multiple auto-antibodies against neuron (one was anti-NMDAR(+), anti-GABABR(+), and the other anti-LGI1(+), anti CASPR2(+). Both patients were adult women with acute onset. Their first symptom was epilepsy, and the treatment effect was good[10].
The clinical significance of multiple auto-antibody has already raised attention of many neurologists and needs to be interpreted in combination with clinical practice. For example, anti-GABABR can be combined with anti-Hu. When anti-GABABR is positive, it is recommended to screen anti-Hu and carry out tumor screening at the same time, such as chest CT, tumor markers, etc., excluding the possibility of tumor as much as possible. In this case chest enhanced CT scan didn’t find tumor, but the patient was advised to take regular examination during follow-up. At present, many reports of anti-NMDAR combined with anti-MOG suggest that it is necessary to consider the clinical syndrome superposition caused by the antibody superposition, pay attention to the clinical process, and inquire in detail the history and imaging data whether there is a basis for demyelination[11].
Table 2 clinical data of AE cases with multiple auto-antibodies
|
N.
|
Sex,
age
|
AE auto-Abs
|
Other Abs
|
Clinical menifestation
|
Brain MRI
|
tumor
|
prognosis
|
|
serum
|
CSF
|
serum
|
CSF
|
|
1
|
M,62
|
GABABR
|
GABABR
|
Hu
|
-
|
Memory loss, somnolence, conculsion, cough, hoarseness
|
Normal
|
Lung cancer
|
Improve
|
|
2
|
M,61
|
GABABR
|
GABABR
|
Hu
|
-
|
Epilepsy, somnolence, memory loss
|
Normal
|
Lung cancer
|
Improve
|
|
3
|
M,59
|
GABABR
|
GABABR
|
Hu
|
Hu
|
Epilepsy, psychosis
|
Lesions of bilateral hippocampus
|
Lung cancer
|
Improve
|
|
4
|
M,58
|
GABABR
|
GABABR
|
Hu
|
Hu
|
Psychosis, memory loss, numbness of limbs
|
Lesions of bilateral hippocampus
|
Lung cancer
|
Improve
|
|
5
|
M,61
|
GABABR
|
GABABR NMDAR
|
Hu
|
-
|
Epilepsy, memory loss, coma
|
ND
|
Lung cancer
|
Improve
|
|
6
|
F,19
|
-
|
NMDAR
|
AQP4
|
AQP4
|
Psychosis, memory loss, blepharoptosis
|
Lesions of bilateral basal ganglia, brainstem
|
No
|
Improve
|
|
7
|
F,40
|
LGI1
CASPR2
|
LGI1
|
-
|
-
|
Myalgia, fasciculation, epilepsy, insomnia
|
Normal
|
No
|
Improve
|
|
8
|
F,56
|
LGI1
|
LGI1
|
Yo
|
Yo
|
Memory loss, conculsion, somnolence, polyphagia
|
Normal
|
No
|
Improve
|
|
9
|
F,50
|
AMPAR
|
AMPAR
|
CV2
|
CV2
|
Memory loss, psychosis
|
Normal
|
Thymoma
|
Improve
|
|
10
|
F,51
|
AMPAR
|
AMPAR
|
Hu
|
-
|
Psychosis, dysphagia, dysdipsia
|
Lesions of bilateral cortex
|
Mediastinal occupying
|
Dead
|
|
11
|
M,44
|
ND
|
GABABR
NMDAR
|
-
|
-
|
Limbic encephalitis
|
Not mentioned
|
No
|
Complete improve
|
|
12
|
F,63
|
-
|
GABABR
|
|
GAD65*
|
Status epilepticus
|
Not mentioned
|
No
|
Dead
|
|
13
|
M,60
|
GABABR
|
GABABR
|
|
SOX1*
|
Limbic encephalitis
|
Not mentioned
|
SCLC
|
Partial recovery
|
|
14
|
M,62
|
GABABR
|
GABABR
|
|
Ri*
|
Limbic encephalitis
|
Not mentioned
|
SCLC
|
-
|
|
15
|
F,68
|
GABABR
|
GABABR
|
|
SOX1*
|
Limbic encephalitis
|
Not mentioned
|
SCLC
|
Partial recovery
|
|
16
|
M,74
|
GABABR
|
ND
|
SOX1
|
ND
|
Limbic encephalitis
|
Not mentioned
|
SCLC
|
Dead
|
|
17
|
M,77
|
GABABR
|
GABABR
|
|
Amphiphysin*
|
Limbic encephalitis
|
Not mentioned
|
SCLC
|
Unresponsive
|
|
18
|
F,57
|
LGI1
NMDAR
|
-
|
-
|
-
|
Faciobrachial dystonic seizure, hyponatremia, mental disorder
|
-
|
No
|
Improve
|
|
19
|
M,66
|
GABABR*
|
|
GAD*
|
|
Seizures, confusion
|
Normal
|
SCLC
|
Not available
|
|
20
|
M,47
|
GABABR*
|
|
SOX1*VGKC
|
|
Seizures, behavior change, memory impairment
|
Bilateral temporal lesions
|
SCLC
|
Partial recovery
|
|
21
|
M,70
|
GABABR*
|
|
GAD*
SOX1
|
|
Seizures, memory impairment, confusion
|
Normal
|
SCLC
|
Unresponsive, dead
|
|
22
|
M,58
|
GABABR*
|
|
Hu*
|
|
Seizures, memory impairment
|
Bilateral temporal lesions
|
SCLC
|
Unresponsive, dead
|
|
23
|
M,61
|
GABABR*
|
|
BRSK2*
|
|
Memory impairment
|
Bilateral temporal lesions
|
SCLC
|
Unresponsive
|
|
24
|
F,57
|
GABABR*
|
|
GAD*
|
|
Subacute cerebellar ataxia
|
Normal
|
Carcinoid of thymus
|
Complete recovery
|
|
25
|
F,30
|
NMDAR GABABR
|
NMDAR
|
-
|
-
|
Epilepsy, psychosis, insomnia
|
Normal
|
No
|
Improve
|
|
26
|
F,43
|
LGI1 CASPR2
|
CASPR2
|
-
|
-
|
Seizures, weight loss, calculation/ memory/speech disorder
|
Bilateral hippocampus/ occipital/parietal lesions
|
No
|
Improve
|
{kind=link}
{kind=link}