Participants and Study Design
A total of 62 women (age range 20–59) were included in this case-control study who presented to our FIRE CLINIC for weight loss treatment for at least 2 months (8 visits) between May 23, 2020 and September 17, 2020 and received CBT-F and pharmacotherapy (n = 42) or pharmacotherapy alone (control group) (n = 20). There was one participant (2.3%) who withdrew from CBT-F and two participants (9.1%) who withdrew from the control group.
We randomly separated participants into CBT-F and pharmacotherapy alone. Average follow-up was 68.5 days. Participants were women with a BMI more than 18.5. In this study, the results are up to phase 1 (8 visits) and phase 2 is being followed up. The results of this time will be a comparison between the baseline and the 8th visit.
The study was approved by the Institutional Ethics Committee of SOUKEN (approval number: 151574_rn-34457. Approved March 1, 2023) and conducted following the principles of the Declaration of Helsinki. All participants were given the opportunity to opt out of participation before initiating this study. Information on the study was posted on the board of FIRE CLINIC to provide participants with the opportunity to opt-out at any time of which the protocol was approved by the institutional review board.
Laboratory data
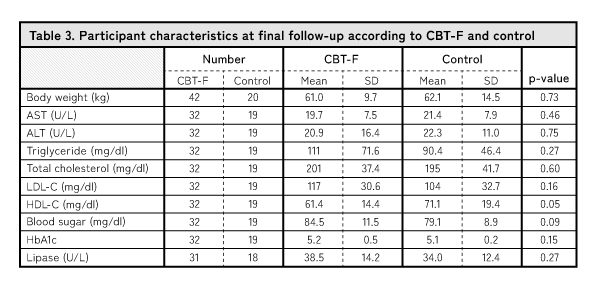
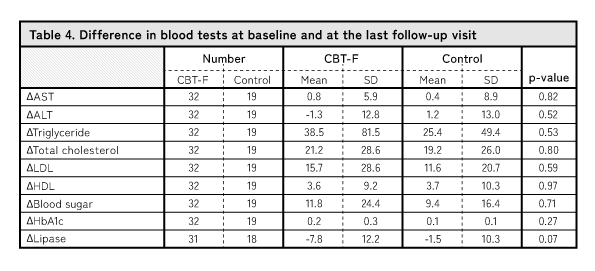
Height was self-reported, and weight were determined using a body composition analyzer (RD-803L-BK, Tanita Corp., Tokyo, Japan). Venous blood samples were collected at the first visit and 8th follow-up. Blood chemistry data [aspartate aminotransferase (AST), alanine aminotransferase (ALT) triglycerides, total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), blood sugar, hemoglobin A1c (HbA1c) and lipase] was outsourced to Health Sciences Research Institute East Japan CO., LTD. Blood was collected in tubes containing ethylenediaminetetraacetic acid and in serum separation tubes for all biochemical tests. The collected samples were kept at room temperature and collected by Insurance Sciences within 1 day and tested within 3 days.
Differences between CBT-F and CBT-OB
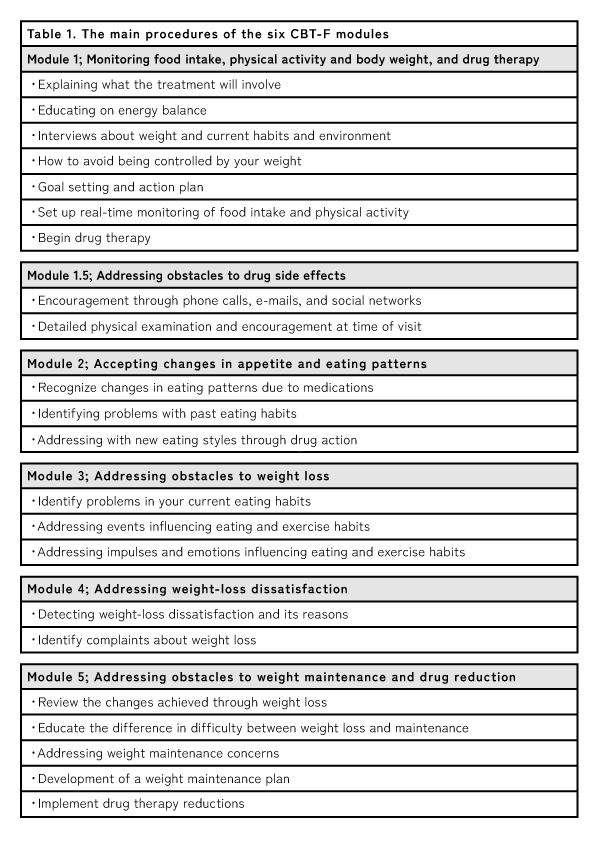
CBT-OB module is shown in Fig. 1 and the CBT-F module is shown in Fig. 2. CBT-F has a different module structure than CBT-OB. Table 1 shows the main procedures of the six CBT-F modules. Although the key difference is the presence or absence of pharmacotherapy, CBT-F has unique modules that result from the concurrent implementation of pharmacotherapy. Module 1.5, which involves addressing obstacles to medication side effects, begins after the completion of Module 1. Module 1.5 deals with obstacles to medication side effects and aims to prevent dropout through online (phone, email, SNS, etc.) or face-to-face encouragement.
In contrast to CBT-OB, which aims at positive changes in eating behavior, Module 2 of CBT-F focuses on retrospective acceptance of changes in appetite and eating behavior resulting from pharmacotherapy. Changes in eating behavior are very important, but they are difficult for patients to grasp, and the barriers are often high due to repeated trial and error. Module 2 of CBT-F focuses on accepting changes in eating behavior caused by medication and adapting to new eating habits. Work with the therapist to become aware of and accept the changes in life that occur when medications suppress appetite and weight loss is observed.
While CBT-OB has a Module 3, " Developing an active lifestyle" there is no equivalent module in CBT-F. This is partly because CBT-F's short- and medium-term programs focus on changing eating behaviors. However, in CBT-F Module 3, " Addressing obstacles to weight loss" there is an opportunity to discuss ways to increase activity when decreased activity is a barrier. This provides guidance on how to increase activity if a patient's activity level is lower than before or if overall activity is decreasing.
Module 4 of CBT-F is equivalent to Module 5 of CBT-OB.
Module 5 of CBT-F aims to reduce the patient's psychological dependence and burden by tapering off medication; CBT-OB is specific to the treatment of bulimia nervosa and other eating disorders, while CBT-F is aimed at those who wish to improve their body shape for the purpose of diabetes prevention, which is the difference is that CBT-F is intended to prevent diabetes and improve body shape.
Medication Therapy
The medications used (Hyguanide, GLP-1 receptor agonist, SGLT2 inhibitor, Bofu-Tsusho-San, Boiogito, Domperidone and Purimperan for anti-nausea, and others) were prescribed according to the physician's judgment as best suited for the patient.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation (SD). Inter-group comparisons were performed using Welch’s t-tests for continuous variables.
All data were analyzed using SPSS version 25 (IBM Corp, Armonk, NY), and p < 0.05 was considered statistically significant.
{kind=link}
{kind=link}
{kind=link}