Cell culture and reagents
The A549 and SK-MES-1 cell lines were purchased from the Shanghai Institute of Cell Biology, Chinese Academy of Sciences and were maintained in RPMI 1640 (Gibco, Grand Island NY, USA; for A549) or EMEM (ATCC 30-2003, Manassas, VA, USA; for SK-MES-1); they were supplemented with 10% FBS (Gibco, Grand Island NY, USA), 100 U/mL penicillin and 0.1 mg/mL streptomycin (Gibco); and were cultured in 5% CO2 at 37°C. The cells were treated with cisplatin (Sigma-Aldrich, St. Louis, MO, USA) for indicated periods of time. Hsa-miR-497-5p mimic, miR-497-5p inhibitor and control mimic or inhibitor were purchased from RiboBio (Guangzhou, China).
Clinical samples
Plasma was collected from 62 NSCLC patients at the Jinling Hospital, Nanjing University School of Medicine from January 2016 to January 2019. The clinicopathological characteristics of the NSCLC patients are summarized in Table 1. The entry standards and standards for objective tumor response for target lesions used in this study were identical to those in our previous study [10]. Front-line chemotherapy for lung Adenocarcinoma (LUAD) comprised cisplatin 75 mg/m2 on day 1, plus gemcitabine 1000 mg/m2 on days 1 and 8, or plus Docetaxel 75 mg/m2 on days 1, every 21 days for 4 cycles. Front-line chemotherapy for LUSC comprised cisplatin 75 mg/m2 on day 1, plus pemetrexed 500 mg/m2 on day 1, or plus Docetaxel 75 mg/m2 on days 1, every 21 days for 4 cycles. Up to 5 ml of blood was collected from patients in a K2EDTA plasma tube (BD Vacutainer, Becton, Dickinson and Company, Franklin Lakes, NJ, USA) and immediately centrifuged (2000g for 10 minutes) within 30 minutes after collection. After separation, plasma samples were transferred to RNase Dnasefree tubes and stored at −80°C until total RNA extraction. All samples were obtained after obtaining written informed consent of patients, in accordance with the Declaration of Helsinki. The study was approved by the Ethics Committee of Jinling Hospital, Nanjing University School of Medicine.
Table 1
Clinicopathological characteristics of participants in this study.
|
|
Resistant (n=30)
|
Sensitive(n=32)
|
P value
|
|
Gender
|
|
|
0.367
|
|
female
|
5
|
9
|
|
|
male
|
25
|
23
|
|
|
Age(year)
|
|
|
0.459
|
|
<65
|
13
|
17
|
|
|
≥65
|
17
|
15
|
|
|
Smoking
|
|
|
1.000
|
|
No
|
13
|
13
|
|
|
Yes
|
13
|
19
|
|
|
Histological type
|
|
|
0.789
|
|
Adenocarcinoma
|
21
|
21
|
|
|
Squamous cell carcinoma
|
9
|
11
|
|
|
Tumor size (cm)
|
|
|
0.069
|
|
<4
|
14
|
23
|
|
|
≥4
|
16
|
9
|
|
|
TNM stage
|
|
|
0.492
|
|
I+II
|
0
|
2
|
|
|
III+IV
|
30
|
30
|
|
RNA extraction and RT-qPCR
RNA extraction from cultured cells was performed using TRIzol reagent (Invitrogen, Grand Island, NY, USA) according to the manufacturer’s protocol. Plasma RNA was extracted using miRNeasy Serum/Plasma Kit (Qiagen, Inc., Valencia, CA) according to the manufacturer’s protocol. cDNA was synthesized with the PrimeScript 1st Strand cDNA Synthesis Kit (Takara Bio, Shiga, Japan) according to the user’s manual. RT-qPCR analysis with gene-specific primers was performed to determine the relative expression of KRT17P3 using SYBR green reagents (Takara Bio) in an ABI 7300 sequence detector (Applied Biosystems, Foster City, CA, USA). GAPDH mRNA was used for normalization. The PCR primers used in this study were: KRT17P3: Forward: 5’-GCCAACACTGAGCTGGAGGTGAAG-3’ and Reverse: 5’-CAATCTGTAGCAGGATGTTGGC-3’; and ACTIN: Forward: 5’-TCATGAAGTGTGACGTGGACAT-3’ and Reverse: 5’- CTCAGGAGGAGCAATGATCTTG-3’.
Cell Counting Kit 8 (CCK8) assay
Cells transfected with plasmid or infected with lentivirus were seeded into 96-well plates at a density of 5×103 cells. After cellular adhesion, medium containing cisplatin at distinct concentrations (0–14 μg/ml) was added to the corresponding cells. After 72h, cell viability was determined by the CCK8 (Donjindo, Kumamoto, Japan) according to the manufacturer’s protocol. Absorbance at 450 nm was measured using a microplate reader (Bio-Tek, Winooski, VT, USA). The IC50 was calculated with Graphpad software.
Cell apoptosis analysis
Cells were treated with different concentration of cisplatin for 24h and were stained with FITC Annexin V and propidium iodide (BD Biosciences) in accordance with the manufacturer’s instructions, and then analyzed by FACScan using CellQuest software (BD Biosciences).
Generation of KRT17P3 knockdown or overexpression cells
Lentivirus harboring shRNA-KRT17P3 and KRT17P3 expression plasmids were constructed by Genechem (Shanghai, China). After 72h infection, the cells were subjected to further studies. Cells infected with lentivirus expressing scrambled shRNA or transfected with a puromycin resistance plasmid were used as control. The targeting sequence of the KRT17P3 shRNA was 5’-TGAACGAGATGCATGAGTA-3’. For the tumorigenicity studies, stable A549 cells with KRT17P3 overexpression were selected in puromycin.
Xenograft animal model
BALB/c nude mice (4-5 weeks old) were maintained on a 12-h light/12-h dark cycle under pathogen-free conditions. After anesthetization, stable KRT17P3-overexpressing A549 cells and control cells (4 × 106) were injected subcutaneously in the back flanks of mice. On day 7 after tumor cell implantation, cisplatin was intraperitoneally injected intravenously (i.p) twice a week. Tumor growth was examined every 7 days for 4 weeks, and the tumor volume was assessed according to the equation: volume = length × width2 × 0.5. All mice were sacrificed, and the xenografts were dissected and weighed for further studies. Animal welfare and experimental procedures were approved by the Institutional Animal Care and Use Committee of Nanjing Medical University.
Western blot analysis
Cells were lysed with RIPA, and 30 μg proteins were separated by SDS-PAGE and transferred to polyvinylidene fluoride membranes. The membranes were blotted with 5% nonfat milk and probed with primary antibodies against anti-PARP-1 (Abcam, Cambridge, MA, USA), anti-mTOR (Abcam) or anti-GAPDH (Santa Cruz, CA, USA), followed by the appropriate secondary antibodies and chemiluminescent detection.
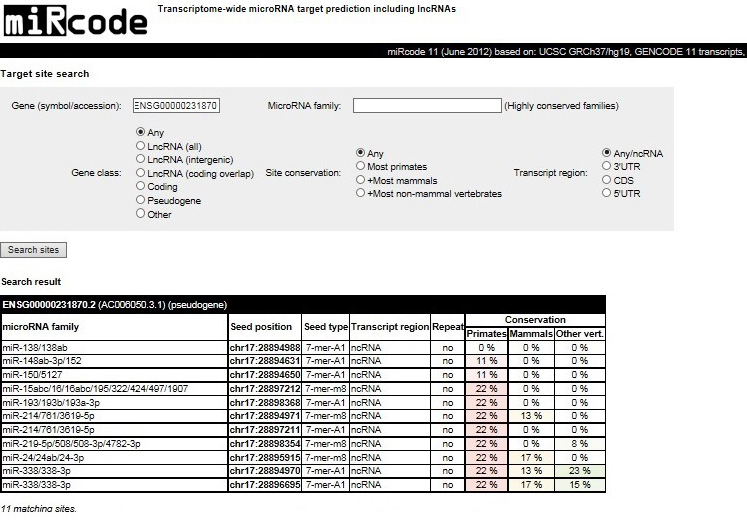
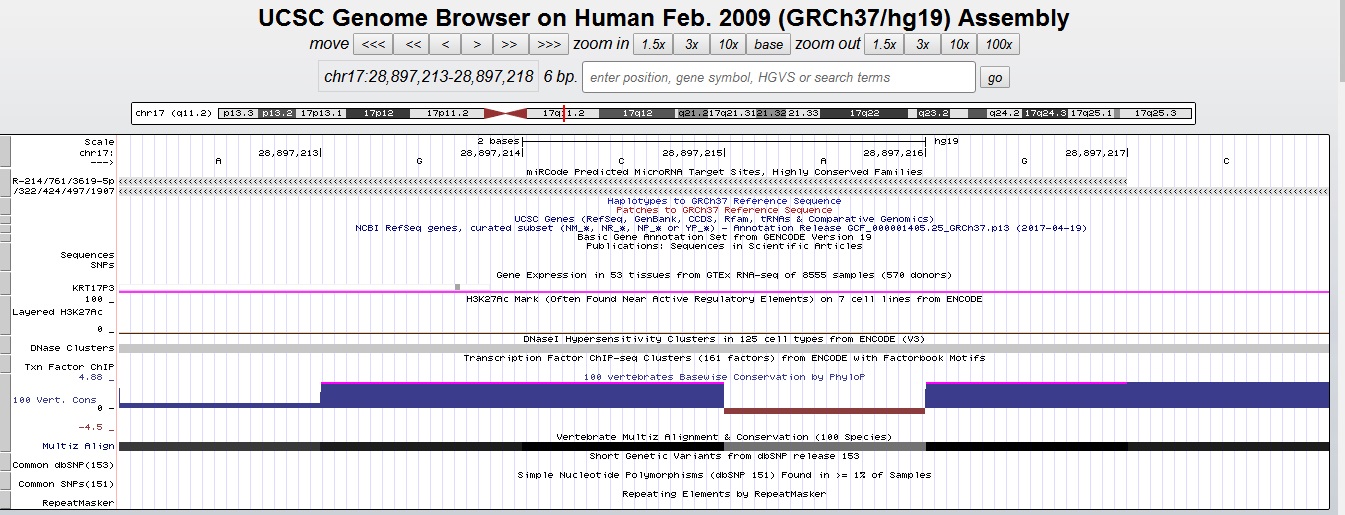
Luciferase reporter assay
The KRT17P3 sequence with a predicted miR-497-5p binding site and the respective mutated sequence were amplified by PCR and inserted into the pmiR-RB-Report vector (Genechem) to construct plasmids KRT17P3-WT and KRT17P3-MUT. These plasmids were then co-transfected into HEK293T cells with miR-497a mimic or mimic-NC. Dual-luciferase assays (Promega, Madison, WI, USA) were performed according to the manufacturer’s instructions.
RNA immunoprecipitation (RIP)
RIP was performed using an EZ-Magna RIP Kit (Millipore, MA, USA) according to the manufacturer’s instructions. Briefly, A549 cells were cotransfected with pKRT17P3 (Genechem) or control plasmid in the presence or absence of pMS2-GFP (Genechem) plasmid and were lysed with RIP lysis buffer. The lysates were incubated with magnetic beads conjugated with anti-GFP (Abcam) or nonspecific control IgG with rotation overnight at 4°C. Then the proteins in the immunoprecipitants were digested with protein K and removed. Finally, the purified RNA was detected by RT-qPCR to measure the level of miR-497-5p. For anti-AGO2 RIP, cells were transfected with pmiR-497 plasmid or control plasmid and were subjected to RIP assays using an AGO2 antibody (Abcam).
Statistical analysis
Statistical analysis was performed with SPSS 20.0 (Abbott Laboratories, IL, USA). All data are presented as means ± SEM. The Student’s t-test was used to analyze data between two groups. The Chi-Square test was applied to examine the clinicopathological characteristics between chemoresistant and chemosensitive patients. The Student’s t-test was applied to the examination of relationship between KRT17P3 levels and clinicopathological characteristics. A value of P<0.05 was considered statistically significant.
{kind=link}
{kind=link}