In the present study, we constructed an immune-related gene pairs signature and validated this signature in the external dataset. Our research showed the signature could stratify patients into low- and high-risk groups. Uni- and multivariate Cox regression analyses showed that the risk score was an independent prognostic factor. The prognostic signature related to tumor immune microenvironment may disclose a new perspective to develop a novel predictive biomarker and improve LGG patient management in the era of immunotherapy.
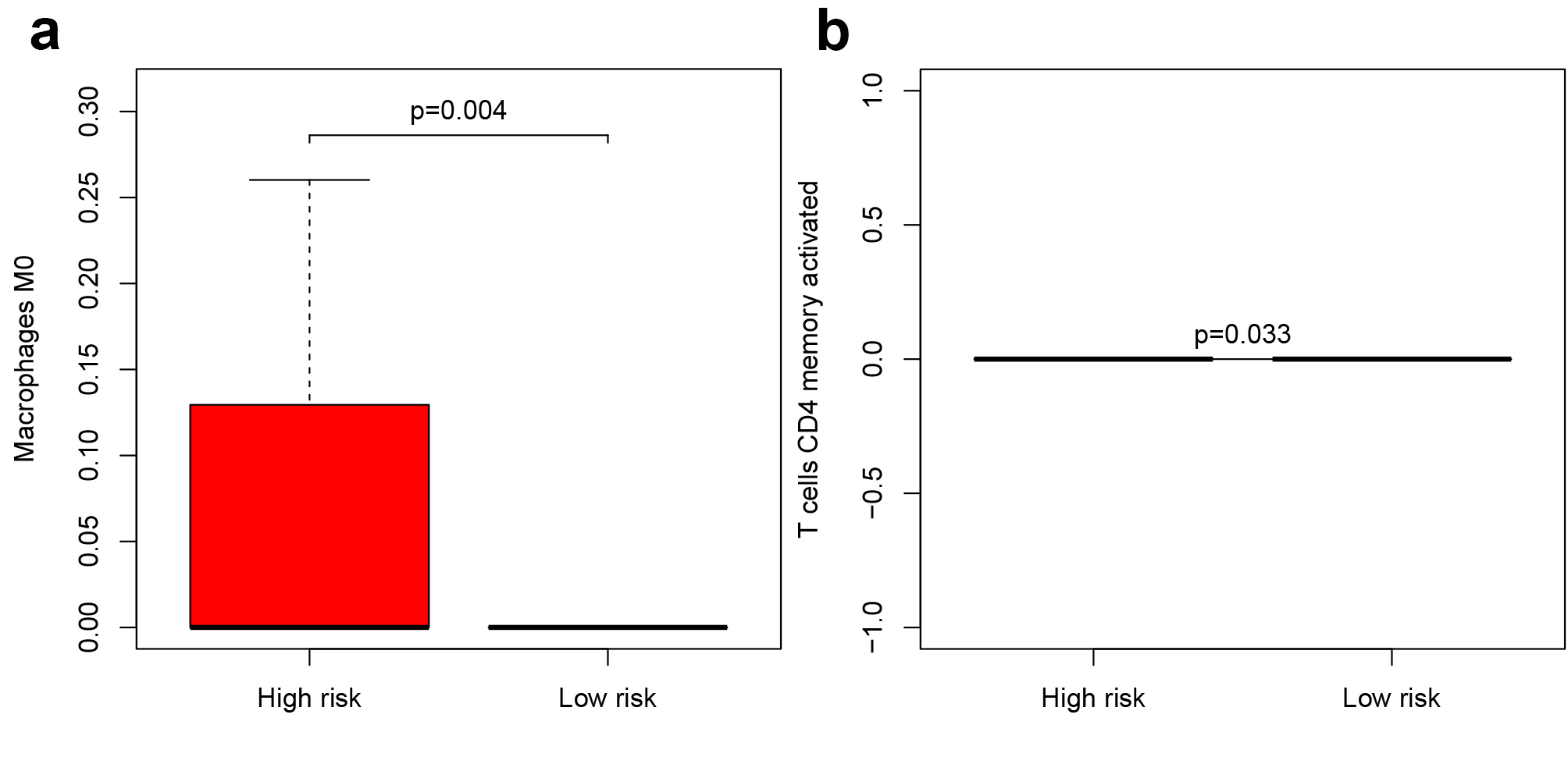
Similar to other studies, several immune cells distributed significantly differently in our research. For example, we found T cells CD8 and Macrophage M0 are significantly enriched in the high-risk group, Wu et al.’ s research[27] also have the same trend, though was not statistically significant. While the opposite view indicated T cells CD8 was significantly higher in the low-risk group[28]. This phenomenon may because the selected immune-related gene pairs and tumor types are different from each other in the above researches. Thus it needs further exploration. Additionally, we filtrated 26 functional pathways from the intersection between GO and GSEA, and this may indicate these immune-related gene pairs take effect through these functions.
Despite a better prognosis for LGG patients (LGGs), 70% of them inevitably progress to high-grade aggressive gliomas and eventually result in death[33]. Over the past 30 years, the overall survival of the majority LGGs had not been significantly improved[2]. Thus, it is vital to develop an individualized treatment protocol for LGG. Reliable prognostic biomarkers could identify patients with poor outcomes and who might benefit from intensive therapy. Recently, significant research on immune-related genes (IRGs) expression has shown great prognostic value in LGG. For example, Deng et al.[34] found up to 397 IRGs were significantly associated with LGG survival. Zhang et al.[21] established a risk model based on 6 IRGs (CANX, HSPA1B, KLRC2, PSMC6, RFXAP, and TAP1). However, one common disadvantage of all the above assays lies in standardizing gene expression profiles, which is difficult to avoid. The immune-related gene pairs signature depends on relative ranking and paired comparison of gene expression profile within a sample. This strategy is in favor of dealing with combined gene expression profiles from multiple databases. LGGs can be further divided into subgroups with different survival outcomes by this prognostic immune signature. So our signature can evaluate LGGs prognosis in a single-sample, individualized form.
Our 8-IRGP signature consists of 15 immune-related genes, and these genes play a vital role in the regulation of the immune microenvironment. Bone morphogenetic protein 2 (MP2) is known to facilitate differentiation and growth inhibition in glioma through the downregulation of both O6-methylguanine-DNA methyltransferase (MGMT) and hypoxia-inducible factor-1a (HIF-1a)[35]. It was reported that killer cell lectin-like receptor subfamily C, member 2 (KLRC2), a transmembrane activating receptor of natural killer cells, expressed higher in glioma-initiating cells compared with neural stem cell lines and normal adult brain tissue[36]. Emerging evidence suggests that the chemokine (C-X-C motif) ligand 12 (CXCL12), which is secreted from glioma stem cells (GSCs), plays a vital role in tumorigenesis and proliferation[37]. Additionally, many of the selected 26 functional pathways are related to the immune microenvironment, such as regulation of immune effector process, positive regulation of cytokine production, and cell chemotaxis. Researches had shown that numerous cytokines and chemokines promote the infiltration of various cells: circulating progenitor cells, endothelial cells, and a range of immune cells such as peripheral macrophages, microglia, leukocytes, CD4 + T cells into the glioma[38–40]. These non-neoplastic cells have an important role in tumor growth, metastasis, as well as response to treatment[14]. Thus these functional pathways matter in glioma immune microenvironment.
There are also some limitations to this study. First, the immune-related gene expression profiles are determined by RNA-seq, which is hard to generalize in daily clinical applications for its sophisticated detection program and high price. Second, the immune signature comes from fresh frozen samples. Thus, there are still doubts about the efficiency and stability. Finally, our study was a retrospective analysis, and prospective research is needed to validate the results.
{kind=link}