Study population
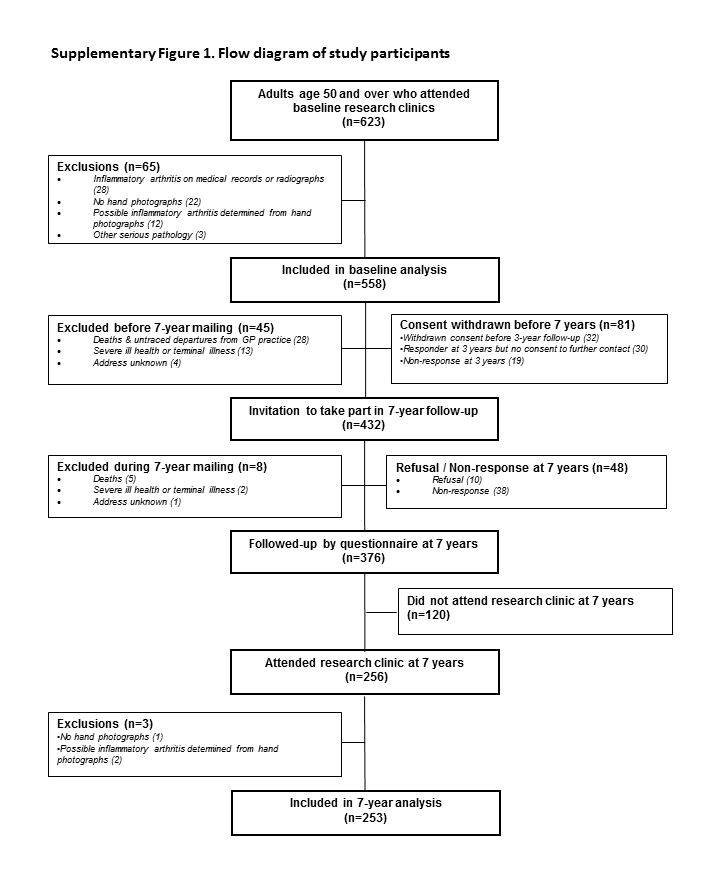
The Clinical Assessment Study of the Hand (CASHA) is a prospective observational cohort study. All individuals aged 50 years and over from two general practice registers in North Staffordshire, UK were invited to participate in a two-stage postal survey that collected data on demographics and characteristics of hand pain and hand problems in 2004-5. Respondents who indicated that they had experienced hand pain or hand problems in the last year were invited to attend a research clinic. Individuals who attended the baseline research clinics were contacted again at 7 years (2011-12) and invited to complete a postal questionnaire and attend a follow-up research clinic. Research clinics at both time points included: digital photographs of the hands, radiographs of the hands and a physical hand examination (13). Seven years was deemed a suitable time period over which some structural progression and soft tissue changes would be seen in a community-dwelling population. Questionnaires at both time points included the Australian/Canadian Hand Osteoarthritis Index (AUSCAN) pain, function and stiffness subscales (14) and at 7 years a question about the perceived change in their hand problem since baseline (15). The study was approved at baseline by North Staffordshire Local Research Ethics Committee (reference: 1430) and at 7-years by West Midlands National Research Ethics Service (reference: 11/WM/0196), and all participants provided written informed consent.
Digital hand photography
Posterior digital photographs were taken of each hand separately using at baseline an Olympus Camedia C-4040 (Resolution 3.8 megapixels (MP)) and at follow-up either a Canon IXUS75 (resolution 7.1MP) or a Canon Powershot A480 (resolution 10.0MP). Hand photographs at both time points were collected in the same standardised position with the camera placed in a fixed position 38 cm (15 inches) above a gridded stand and were comparable to those used in the AGES-Reykjavik photographic scoring system (9). The participants were seated with their shoulder adducted and the elbow flexed to 90O. The hand was pronated and placed in a fixed position on the gridded stand with forearm, wrist and fingers in a straight line and the hand resting in a natural position, i.e. with the fingers and thumb not held closely together or spanned. Figure 1 provides an example of the images taken at baseline and 7 years for a participant.
An experienced reader (HJ) who was blinded to the clinical and radiographic data graded photographs from baseline and 7 years using the AGES-Reykjavik photographic scoring system. As per the scoring system, the presence and severity of hand OA were graded on unpaired photographs but with a known time sequence (chronological) (9). Five joints in each hand (second and third distal interphalangeal (DIP), second and third proximal interphalangeal (PIP) and first carpometacarpal (CMC) joints were examined visually for the presence of hard tissue (bony) enlargement, deformity and nodes. While OA is not restricted to these joints, for feasibility they were selected for examination in this study as they are the joints assessed in the clinical ACR hand OA criteria. Each joint was given a score on a 0-3 scale, with the assistance of a reference photographic collection, where 0 = normal: no evidence of OA, 1 = mild: some evidence of OA but not fulfilling the criteria for definite disease, 2 = definite: moderate OA and 3 = severe OA. Joint groups across both hands (DIP, PIP and CMC joints) were also graded using the same 0-3 scale with the highest scoring joint determining the grade for a joint group. Hand OA on digital photographs was defined as being present in a joint or joint group if the grade was ≥2.
For the purpose of assessing reliability, a second experienced reader (GPH), also blinded to the clinical and radiographic data and the scores of the first reader, scored all the 7-year hand photographs (n=253) to determine inter-rater reliability. Intra-rater reliability was determined by (HJ) reading a sample of the hand photographs (n=30) for a second time after at least four weeks.
Radiographic scoring
Dorsipalmar (DP) radiographs of the hands and wrists were taken at baseline and 7-year follow-up according to a standardised protocol (13). A single reader (MM), blinded to all questionnaire, clinical assessment and photographic data, graded all the baseline and 7-year hand radiographs unpaired with known chronological order. The presence and severity of OA using the Kellgren and Lawrence (KL) grading scale (0-4) was used to assess the second and third DIP, second and third PIP and first CMC joints in each hand (16).
Intra-rater reliability for the presence of hand OA in a joint was found to be excellent (mean Kappa (K)=0.85 and percentage exact agreement (PEA)=95%). Inter-rater reliability had previously been established with a second reader, an academic rheumatologist (RD) and found to be good (mean K=0.79 and PEA=95%) (17).
Physical examination
Physical examination of the hands was undertaken at baseline and follow-up research clinics by trained physiotherapists and occupational therapists. The presence of nodes, hard tissue (bony) enlargement and deformity was determined in the second and third DIP, second and third PIP and first CMC joints in each hand and also any swelling present in the metacarpophalangeal (MCP) joints were recorded. Whilst we did not undertake formal reliability testing of the physical assessment in the study at baseline and 7 years, quality assurance and control were integral parts of the study as detailed in the study protocol (13). Clinical assessors, qualified occupational and physiotherapists, underwent training for the physical assessment techniques. A detailed Assessors Manual with protocols for physical assessment was provided to assessors for reference during the study and quality control sessions were undertaken at regular intervals throughout the study. Therapists were not aware of the photographic or radiographic scores as these were determined after the research clinics had taken place.
Exclusions
Participants were excluded from this analysis if they did not have digital hand photographs at both baseline and 7-year follow-up and if general practice or local rheumatology medical records or a musculoskeletal radiologist identified them as having inflammatory arthritis (rheumatoid or psoriatic arthritis) at baseline. They were also excluded if there was an indication of possible inflammatory arthritis or other serious pathology (scleroderma, neuropathic changes or severe contracture) on the digital hand photographs at baseline or 7-year follow-up, as determined by a consultant rheumatologist (HJ). Additionally, if a participant reached the maximum score at baseline for the photographic, radiographic scores or the maximum number of clinical features, then they were excluded from selected joint and person-level analyses as they were unable to progress.
Statistical analysis
Reliability of using the photographic scoring system has previously been established (11), thus reliability was undertaken at 7-years to ensure that this hadn’t markedly changed. The inter-rater reliability of the scoring of photographic hand OA at 7 years was assessed across all participants using intra-class correlation coefficients (ICC), using 2-way random effects models with absolute agreement, for the 10 hand joints and three joint groups. Intra-rater reliability was also assessed, to ensure consistency of scoring by the main observer (HJ), in a randomly selected sample (n=30) using ICCs for the three joint groups.
No reference standard is available for assessing progression on digital hand photographs so examining criterion validity was not possible. Therefore, longitudinal construct validity was investigated against a number of constructs. At the joint and joint group level the proportion of individuals who had shown photographic hand OA progression deom baseline to 7 years (increase in score ≥1) was calculated for individuals i) with (increase in score of ≥1) and without (change in score of <1) radiographic progression between baseline and 7 years and ii) with (increase in score of ≥1) and without (change in score of <1) progression of clinical features between baseline and 7 years. For a joint group, the highest change in in any joint between baseline and 7 years that was present within a joint group was used for photographic OA, radiographic OA and the number of clinical features. In addition, change scores were also calculated to represent the magnitude of change at each joint and in each joint group (7-year follow-up score – baseline score) for each construct (photographic, radiographic, clinical features). As data were not normally distributed, Spearman Rank correlation coefficients were used to assess how similar the constructs of radiographic OA and number of clinical features present were to the hand photographic scoring. Two a priori hypotheses were set regarding these correlations at the joint and joint group level:
1) Change in photographic hand OA scores for each joint was expected to correlate more closely with the change in the number of clinical features than with the change in radiographic OA grade. 2) Correlations would be the same or slightly lower than was achieved at baseline for cross-sectional construct validity in each hand joint and joint group (11).
At the person-level photographic hand OA scores were summed for the 10 assessed hand joints and change scores calculated (7 year – baseline; max range -30 to 30). Individuals were divided into tertiles based on the distribution of data and categorised into those that had not progressed (change score ≤0), those that had undergone mild progression (change score = 1 to 2) and those that had undergone at least moderate progression (change score ≥3). Additionally, the number of joints that had undergone photographic hand OA progression over 7 years was examined using tertiles based on the distribution of data and categorised into no progression (0 joints), mild progression (1-2 joints) and at least moderate progression (≥3 joints). Analysis of variance was used to describe the mean (and 95% confidence intervals (CI)) summed radiographic OA score at 7-years, summed number of clinical features at 7-years, and 7-year AUSCAN pain (0-20), function (0-36), stiffness (0-4) and total (0-60) scores adjusted for baseline score for each tertile and to test for significance of differences between the tertiles and determine if change over time was similar between the different constructs. Percentages and Chi-Square Tests were used to explore differences in individuals perceived global assessment of change in their hand problem over 7-years (improved, no change, deteriorated) between the tertiles.
{kind=link}