The patient is a 65-year-old Chinese woman with a 4-year history of hypertension, and a 14 months history of proteinuria and microscopic hematuria. The patient had been in her baseline renal condition until January 9, 2020. As shown in Table 1, her baseline estimated glomerular filtration rate (eGFR) in the past year range from 64.2 ml/min/1.73m2 to 72.6 ml/min/1.73m2. Baseline urine sediment examination showed 36.61 cells/ml -74.43 cells/ml in erythrocyte count and baseline proteinuria excretion was up to 510 mg/day. Three days prior to her admission, she got flu-like symptoms including headache, myalgia and fatigue, which were resolved in 1 to 2 days. However, she developed dark-colored urine and flank pain a day later and presented to the out-patient clinic. Urine sediment investigation showed significant worsening in urine erythrocyte count (2518.03/mL) and she was admitted to the hospital on January 10, 2020. On admission, vital signs were normal with a body temperature of 36.8°C, blood pressure of 149/104 mm Hg, heart rate of 80 beats per minute, and a respiratory rate of 16 breaths per minute. Both lungs were clear to auscultation. The rest of the physical examination was also unremarkable.
Table 1 Laboratory characteristics of the patient
|
Date
|
2019.1.25
|
2019.3.18
|
2019.5.22
|
2019.9.23
|
2020.1.9
|
2020.1.10
|
2020.1.20
|
2020.1.25
|
2020.4.20
|
Reference range
|
|
RBC
|
70.4
|
NA
|
NA
|
36.6
|
2518.0
|
98.9
|
NA
|
NA
|
28.3
|
0-30
|
|
Proteinuria excretion, grams/24 hours
|
0.51
|
0.45
|
0.27
|
0.43
|
NA
|
1.07
|
NA
|
NA
|
NA
|
£140
|
|
Creatinine, mmol/L
|
83
|
75
|
80
|
75
|
84
|
96
|
74
|
79
|
73
|
45-84
|
|
eGFR, ml/min/1.73m2
|
64.2
|
72.6
|
67.1
|
72.1
|
62.8
|
53.6
|
73.5
|
67.9
|
74.7
|
>90
|
|
UACR, mg/g
|
43.6
|
NA
|
NA
|
36.1
|
NA
|
288.8
|
NA
|
NA
|
33.61
|
0-30
|
|
WBC, x 109/L
|
NA
|
NA
|
NA
|
NA
|
NA
|
4.57
|
4.58
|
7.45
|
5.72
|
3.5-9.5
|
|
Lymphocyte count, 109/L
|
NA
|
NA
|
NA
|
NA
|
NA
|
0.86
|
0.81
|
1.05
|
1.34
|
1.1-3.2
|
|
Lymphocyte percentage, %
|
NA
|
NA
|
NA
|
NA
|
NA
|
18.8
|
17.8
|
14.1
|
23.4
|
20-50
|
|
hs-CRP, mg/L
|
NA
|
NA
|
NA
|
NA
|
NA
|
19.6
|
36.6
|
4.6
|
NA
|
NA
|
RBC: urine red blood cell count; WBC: blood white blood cell; eGFR: estimated glomerular filtration rate; hs-CRP: hyper-sensitive C reaction protein; UACR: urine albumin to creatinine ratio; NA: not applied.
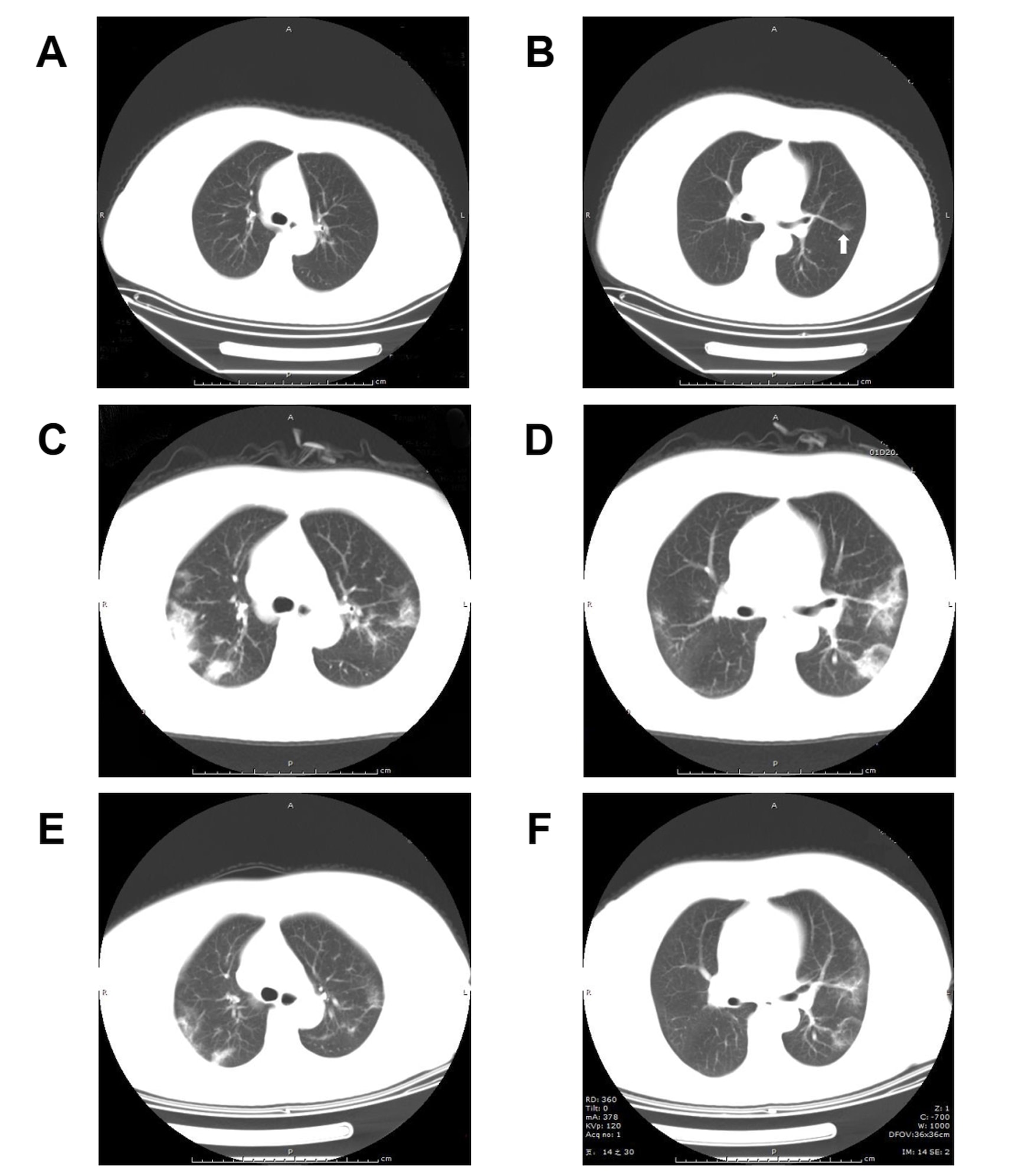
Laboratory results from the time of admission are summarized in Table 1. She got decreased eGFR (53.6 ml/min/1.73m2) and deteriorated proteinuria (1.07 g/day) when compared to her baseline level. Notably, the patient had mild lymphopenia and increased C reaction protein level. Serologic examinations for hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodeficiency virus (HIV) were negative. Anti-nuclear antibody, anti-extractable nuclear antigen antibodies, anti-neutrophil cytoplasm antibodies and anti-glomerular basement membrane antibody were negative. Serum immunoglobulin (Ig) A level was slightly increased at 4.71 g/L (reference range: 0.82 g/L-4.53 g/L), whereas IgG, IgM, complement C3 and C4 levels were within the normal range. An ultrasound and a Computed tomography (CT) examinations for the urinary system were unremarkable. A chest CT scan revealed scattered ground glass opacity (GGO) (Fig. 1A and 1B).
On admission day 5, a renal biopsy was performed. A total of 16 glomeruli were identified in the tissue submitted for evaluation, 5 of which were completely sclerosed. One glomerulus showed segmental sclerosis and one showed a fibrocellular crescent (Fig. 2A). Focal mild mesangial hypercellularity is identified in rare glomeruli. There is no evidence of significant glomerular inflammation or necrosis. The tubular parenchyma showed moderate interstitial fibrosis associated with nonspecific mononuclear cell inflammatory. Intact tubules showed focal acute tubular injurious changes characterized by attenuation of the brush borders and cytoplasmic vacuolization as well as luminal cellular debris (Fig. 2A and 2B). By immunofluorescence microscopy, the glomeruli showed 2+ granular mesangial staining for IgA (Fig. 2C), C3, kappa and lambda light chains. IgG, IgM and C1q were negative. Electron microscopy (EM) examination revealed mesangial electron dense immune-type deposits. There is no evidence of definitive viral particles (Fig. 2D). A diagnosis of IgA nephropathy with an Oxford score of M0E0S1T1C1 was rendered.
With the diagnosis of IgA nephropathy, she received valsartan, an angiotensin II receptor blocker (ARB), with an initial dosage of 20 mg per day. She experienced dry cough without fever, dyspnea, diarrhea, myalgia or sore throat on admission day 12. Consequently, we repeated a chest CT scan for her out of caution due to COVID-19. The CT images showed a significant interval progression with a viral pneumonia pattern (Fig. 1C and 1D). A panel of infectious disease screening was initiated including IgM antibodies against nine respiratory pathogens: influenza virus A, influenza virus B, parainfluenza virus, adenovirus, respiratory syncytial virus, pneumonophagous legionella, Q fever rickettsia, mycoplasma pneumoniae and chlamydia pneumoniae, which were all negative. A throat swab specimen tested positive for SARS-CoV-2 later. TLhe frozen renal tissue from biopsy specimens was submitted for reverse transcription-polymerase chain reaction, however, which was tested negative for SARS-CoV-2. Immunohistochemical (IHC) evaluation for the spike protein (40150-R007, Sino Biological, Beijing, China) of SARS-CoV-2 in the kidney was negative as well (Fig. 2E). According to the guildline for COVID-19 issued by the National Health Commission of China (8), she received methylprednisolone (40 mg per day for 3 days) and empirical anti-virus medication (oseltamivir at 75mg, twice a day for 5 days).
On admission day 17, a follow-up chest CT scan showed a significant improvement (Fig. 1E and 1F). Laboratory investigations showed stable renal function and restored lymphocyte count (Table.1). A repeated throat swab specimen tested negative for SARS-CoV-2. The patient was discharged.
Three months later, the patient remains asymptomatic clinically. A follow-up investigation revealed positive IgG and the IgM antibody against SARS-CoV-2. Her eGFR and UACR were 74.69 ml/min/1.73m2 and 33.61mg/g respectively; her urine erythrocyte was 28.3 cells/ml (her baseline level). The valsartan dosage was titrated to 40 mg OD for optimizing her blood pressure control.
{kind=link}