As of June 1, 2020, coronavirus disease 2019 (Covid-19) has been confirmed in ~ 6,000,000 people worldwide, carrying a mortality of approximately 6.8% [1], compared with a mortality rate of less than 1% from influenza. Italy (especially Northern Italy) has been badly it by the epidemic in the March-April period [Fig. 1 – Fig. 2]. The epidemic in January was mainly restricted to China and few cases in South-East Asia (Thailand, Malaysia, Singapore, Taiwan, Japan and South Korea) and in Europe (France and Germany) [2]. Almost a month later, on February 16th, the first COVID-19 was identified in Italy at Codogno Hospital (Lodi) [3]. In few days two outbreak sites were identified 15 cases in Lodi (Lombardy) and 4 cases in Vo’ (Veneto) and on Feb 21st the first Italian COVID-19 died in Padua [4]. On March 8th the Italian epidemic became the second largest in the world behind Korea (outside of mainland China) and the largest in the Western countries in terms of COVID-19 confirmed cases with 6,387 cases, including 366 deaths. The majority of these cases were located in northern regions, with Lombardy and Emilia Romagna reporting a combined 5,369 cases (84%). The Italian government, consequently took a number of steps in an attempt to limit the spread of SARS-CoV-2 and over the weekend, cordoned a region containing almost a quarter of all Italian citizens The measures did not permit the travel in or out of Lombardy and other surrounding towns, except for proven work or emergency-related reasons [5].
On March 10th in Italy, Europe’s worst affected country, total confirmed cases jumped to 9,172 with 463 deaths, making it the 1st largest outbreak outside of mainland China. The Prime Minister expanded movement restrictions to the entire country. The decision came after a spike in deaths from COVID-19. The measures include cancellation of all public gatherings, restriction of movement throughout the country, and an extension of school and university closures through at least the next month [6]. On March 12th the Italian Ministry of Health reported a total of 12,839 cases and 1,016 deaths. The New York Times reported that Italy’s health system has become rapidly overwhelmed in just 3 weeks, leading to severely limited availability for ventilators and necessitating difficult decisions regarding how ration medical care among patients. The rapid spread and increase in the number of severe cases prompted Italy to enforce radical social distancing measures and to strongly encourage other countries to rapidly implement these measures as well [7]. On March 19th Italy has overtaken China with respect to the number of reported COVID-19 deaths, reporting a total of 3,405 deaths compared to 3,248 reported deaths in China; however, China’s 80,967 cases remained the highest national total, and Italy is second with 33,190 [8]. The speed of the epidemic and the associated damages were evident from the first week of March [Fig. 1] and the Hospital management (lead coordinated by the General Director), worried about the risk of the fragile patients present in the Cancer Institute, for their age and their comorbidity, started to elaborate possible COVID-19 therapeutic strategies as well as established the COVID-19 Crisis Unit, coordinated by the Medical Director. The therapeutic strategy based on inhibition of IL-6R has been previously published [9–11] and will not be furthermore elaborate in this article, which will be focused on the strategies adopted to prevent COVID-19 spreading among the susceptible cancer patients and their care givers, as well as the Cancer Institute Health workers. Moreover, the IRCCS Pascale under the coordination of the Scientific Director participated to COVID-19 Research Programs launched by the Campania Regional Government, as well as by the Italian Ministry of Health.
The mission of a comprehensive Cancer Center in a country with implementation of an advanced welfare and universal health system (adopted in Italy since 1978), besides implementing translational research and clinical trials with the most innovative treatment, must include cancer prevention research and territorial Regional coordination of cancer early diagnosis and follow-up programs (in Campania the Oncological Network is coordinated by the INT Pascale since 2017). The organization in Departments dedicated to specific cancers (i.e. breast and head and neck cancers) and multidisciplinary and integrated teams (GOM, multispecialty oncological groups, made by oncologists, surgeons, radiotherapist, radiologists, pathologists, biologists and virologists, depending on the cancer type and etiology) accelerated the involvement of the whole Institute also in the COVID-19 emergency. In a contest where research, patient clinical care and health management within a global multidisciplinary philosophy are contributing to improving health programs and outcomes, the COVID-19 pandemic had to be tackled according to an unprecedented knowledge management and innovation approach [12, 13], which allows research, clinical science and management to stimulate each other to achieve a synergistic collective intelligence [14] and even a global collective intelligence [15].
The COVID-19 activities at the INT-Pascale
The major areas of translational research pursued at the Pascale Institute have been aimed at identifying the mechanisms underlying the pathogenesis of COVID-19 to improve diagnostic and therapeutic approaches to this disease. In particular, the following activities have been focused on:
1) The construction of a regional database in which to record all the COVID-19 cases in order to analyze the correlation between biomarkers and clinical-pathological characteristics;
2) The start of a monitoring activity for the spread of the epidemic among health workers;
3) Sequencing of the SARS-CoV-2 virus to monitor possible evolution;
4) Characterization of the immune response to SARS-CoV-2;
5) The study of the role of innate immunity and the ACE2 receptor in SARS-CoV-2 infection;
6) The characterization of mediators of the inflammation in patients with COVID-19.
The Institute decision to ensure continuous commitment to and treatment of cancer patients determined the reorganization of most clinical oncology activities in the medical and the surgical oncology wards as well as in diagnostic units and the sectors dealing mainly with not hospitalized patients (i.e. radiotherapy and interventional radiology).
COVID-19 impact on Medical Oncology (P.Ascierto and S.Pignata)
The Istituto Nazionale Tumori of Naples has a major focus on cancer molecular characterization, biomarkers identification and implementation of tailored precision medicine with the backing of innovative therapeutic strategies. In line with this strategy, the Institute and their clinical units are members of several networks contributing and coordinating several national and international European clinical trials for different type of cancers. Most conventional and palliative treatments are left to smaller oncology units distributed in the Campania Region, which are part of the regional oncology network, coordinated by the Pascale Cancer Institute.
In the 50-day period (March 10th -April 30th ) the COVID-19 pandemic heavily influenced the conduction of clinical trials at the Pascale Institute, as in many other European countries, by the excess load in Intensive and sub-intensive care units (ICU) of COVID-19 patients affected by severe respiratory syndrome (ARDS). Moreover, the clinical trial conduction has been severely hampered by the national lockdown, with limitation of patients and caregivers free circulation, and even more by the severe restriction imposed by the Campania Governor in order to achieve social distancing by the home isolation for the all population
Our institute, however, maintained a strong commitment to reduce the impact of COVID-19 on ongoing clinical trials and, in agreement with regulatory agencies, pursued their pivotal principals: assuring the safety of trial participants; - maintaining compliance with good clinical practice (GCP); - minimizing risks to trial integrity and quality of data. Although with varying difficulties, most of the Pascale clinical research team, in line with the national regulatory agency AIFA and the EMA, adopted the following general rules:
1. Continuation of multicenter clinical trials coordinated by the Pascale Institute.
In accordance with AIFA, the following recommendations were issued to continue clinical trials in centers where possible and to prepare a specific risk plan. In particular:
-
- give instructions to the sites on how to proceed for enrollment, investigational medical product (IMP) and visits;
-
- check the IMP stock at the sites;
-
- contact the couriers to guarantee the delivery of IMP;
-
- continue to include patients in ongoing trials with open recruitment at internal and external sites if they can guarantee the standard health care of the patient in case of any complication related to the disease, the IMP or the COVID-19 infection, as well as the compliance with the protocol
-
2. Participation of Pascale Units to protocols coordinated by other groups or Pharma
Patients already signed the Informed consent form should be included in the trial as far as the patient fulfills all the inclusion criteria and none of the exclusion criteria. New patients can be also considered.
IMP should not be stopped unless there is an issue with access to drug or concern regarding the possibility of providing the optimal health care to the patient. In the latter it can be considered a return to standard treatment.
Management of COVID + patients enrolled in a clinical trial is expected to follow the regular protocols. In symptomatic patients, IMP must be postponed until the patient’s recovery. In the case of asymptomatic COVID + patients, it is reasonable to delay IMP administration until the patient will become COVID negative or 14 days has passed without symptoms.
For oral drugs, taking into consideration the restrictions in mobility for patients and with the aim of reducing pontetial patients’ exposure to COVID-19, it could be choice to dispense and shiporal IMP to the patient by courier or mail, if possible in some trials. In this case, a clinical assessment before continuing oral IMP is mandatory and may be carried out by phone or videoconsultation and documented in the medical record.
The communication of the blood results can be done by teleconsultation. When the patient is not able to visit the hospital, it should be considered to take the blood tests in another facility close to the patient and inform the result to the investigator by teleconsultation.
It is also recommended to maintain the recruitment of PRO questionnaires during this period.
The investigators are strongly encouraged to contact the Sponsor information about any circumstances that may impact the management of the trial at sites during the COVID-19 pandemic in order to set up a mitigation plan. This is especially relevant if halt to recruitment or patients discontinuing trial treatment is considered. The investigator and the sponsor are invited to find the best solution for the patient, even delaying the IMP administration or even transferring the patient to another site.
In order to limit COVID 19 spread and to guarantee continuity of cancer care, some suggestions have been given by a board of Italian oncologists belonging to main scientific societies (AIOM, CIPOMO and COMU) [16].
According to these advices, it was suggested to carefully balance risks and benefits of oncological therapies and to prioritize treatment during this pandemia. In clinical practice, one possible strategy could be to delay, as far as possible, adjuvant treatments or to prefer schedule with longer interval (this is what it was also recommended by ESMO for melanoma) [17].
Telemedicine could be used in patients in immunotherapy, or in treatment with weekly chemotherapy, or in maintenance therapy, performing blood tests in laboratory near to patient’s home, and with medical assessment by phone. This approach could also be used in patients in follow up with no evidence of recurrence at radiological exams telematically checked.
If it is not necessary, it should be avoided the access of caregivers at scheduled therapy visit and in day hospital area, where treatment is administered. It is deeply suggested to forbid access of patient with respiratory syndrome or with fever who have not undergone any previous triage; in these patients strongly we recommend to perform a nasal swab to ascertain the possibility of a COVID-19.
Another issue is differential diagnosis in patients with suspicious respiratory symptoms undergoing immunotherapy or other drugs that can cause as adverse event interstitial pneumonia, or in patients on treatment with BRAFi/MEK inhibitors affected by fever that does not resolve with treatment interruption. In these cases, we should require a COVID test.
Considering data available on cancer patients and COVID 19 [18, 19], oncological decisions during this pandemia should be taken prudently and according to the latest evidences and scientific recommendations.
COVID-19 impact on Surgical Oncology
The major impact of COVID-19 within the surgery oncology activities is mainly on the respiratory and gastro-digestive tract for the direct infection of lining epithelial and organs by the SARS-CoV-2. Specific epithelial cells of both districts (i.e. epithelial cells of lung alveoli and bile ducts) have on the surface glycoprotein ACE2 molecules, which represent the binding site (receptor) for the viral Spike molecules. The Angiotensin-converting enzyme 2 (ACE2) is an enzyme attached to the outer surface (cell membranes) of cells in the lungs, arteries, heart, kidney, and intestines. ACE2 lowers blood pressure by catalysing the hydrolysis of angiotensin II (a vasoconstrictor peptide) into angiotensin (1–7) (a vasodilator). ACE2 counters the activity of the related angiotensin-converting enzyme (ACE) by reducing the amount of angiotensin-II and increasing Ang(1–7). For such reason specific precautions must be taken during the surgery as well as during the post-surgery curettage/ bandaging for outpatient treatment, in particular of tracheostomy or colostomy patients.
Surgical Oncology of the Head and Neck District During Covid-19 Pandemic
The main mechanism of transmission of COVID-19 is through the air, followed by, to a lesser extent, direct or close contact and finally by the fecal-oral route. Transmission is generally realized through contact with a symptomatic case, but it also possible from an asymptomatic infected subject. For this reason, health care workers who come into contact with the upper aerodigestive tract during diagnostic and therapeutic procedures - such as otolaryngologists, head and neck surgeons, oral and maxillofacial surgeons and dentists - are particularly at risk because of the rapid spread of this disease through respiratory droplets [20, 21].
Moreover, all Head and Neck inspections are considered high-risk procedures and, given the risk of contagion from completely asymptomatic patients during this pandemic, every patient must be considered a possible cause of transmission. Therefore, it is mandatory to adopt the right precautions during patients’ clinical inspection, and, subsequently, during hospitalization/intra-operative/post-surgical time.
Based on the experience gained in Wuhan, China, and Northern Italy, it was evident that N95 masks were not sufficient to control the dissemination of the disease. Indeed, it was not until PAPR (Powered Air Respiratory Protection) was introduced that the transmission of the virus was controlled among medical personnel [21].
During ENT examination with flexible laryngoscope, in order to reduce nausea and irrigated cough, the smallest possible laryngoscope diameter was employed associated to the use of anaesthetic gel, that replaced local anaesthetic spray [22]. For each patient we used a disposable device that covers the endoscope. The same procedure was performed during nasal fibroendoscopy, to ensure adequate surface anaesthesia in the way of reducing sneeze reflex. All endoscopic procedures were performed safely both for operators and patients.
High-risk operations were performed with appropriate PPE worn by the health care personnel. Considering the high viral titles in nasal mucosal and oral, pharyngeal, and pulmonary secretions, every intervention that involves these surfaces/fluids is at high-risk to the entire operating room personnel. This includes the use of powered devices (eg, drills, microdebriders, saws) or ultrasonic shears, such as the Harmonic scalpel (Ethicon) or Thunderbeat scalpel (Olympus).
In every surgical procedure, coordination with the anaesthesia team was crucial. During the intubation or the extubation, only personnel considered essential to the procedure remained in the surgical room, while all non-essential staff leaved the room and returned after the airway was secured.
We also payed particular attention and used adequate protection when transferring patients. Clear protocols were established with the anaesthesia department, nursing staff, recovery unit personnel and infection control team .
Adequate protection when transferring patients is critical. Non-intubated patients were transferred while wearing a surgical mask. The administration of oxygen was performed by face mask over the surgical mask. Intubated patients were transported with an ICU ventilator (dry circuit, filter in place) in order not to interrupt the closed circuit. Each healthcare professional participating in the patient transfer wore a PPE. Also nurses operating postoperative care are given PPE.
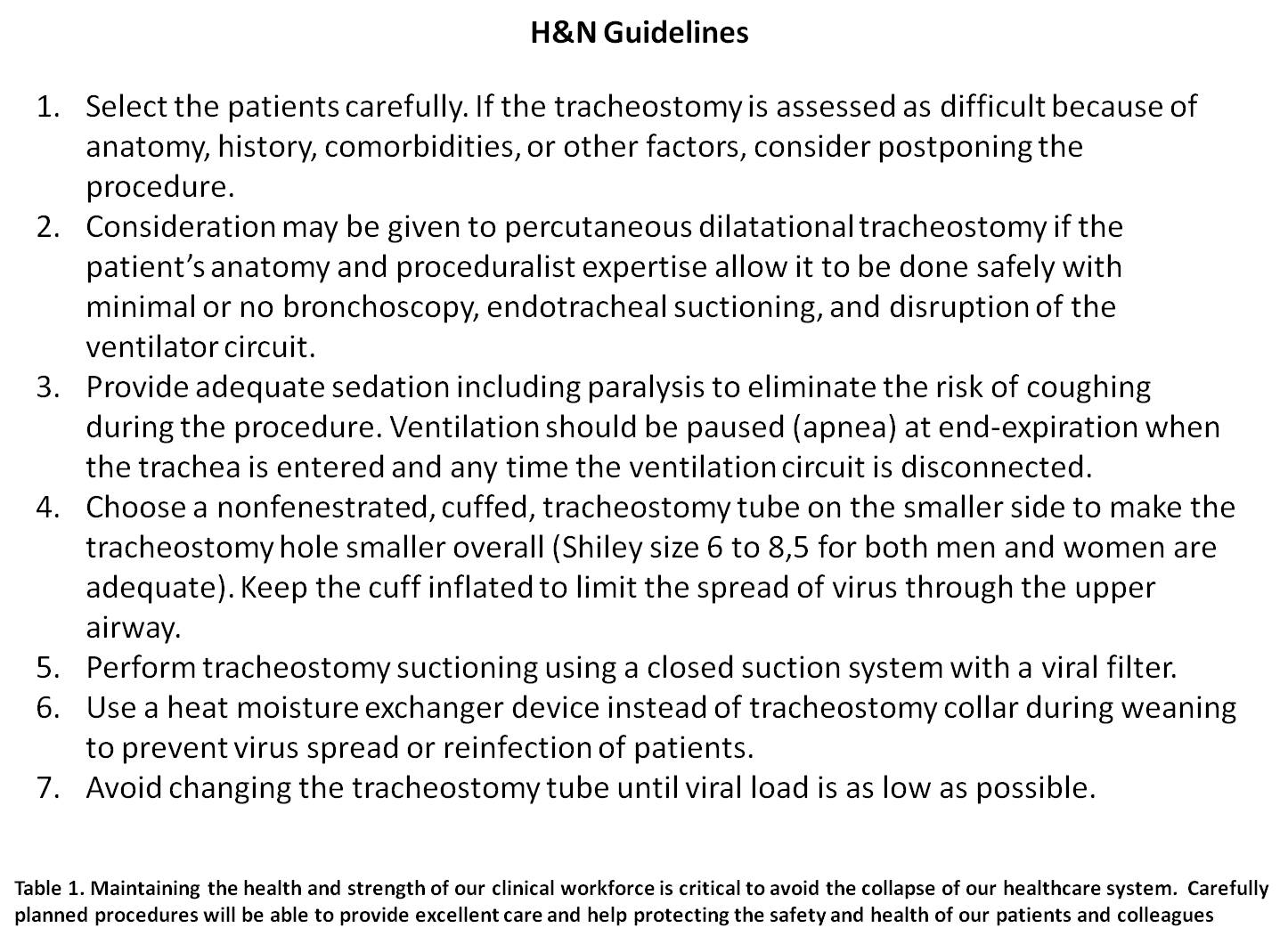
A special attention was dedicated to tracheotomised patients. In these cases, a closed aspiration system was used to minimize secretions during nursing procedures. In this specific time cancer patient management became an even more difficult challenge given that cancer patients represent a high-risk group in the COVID-19 pandemic emergency. These patients are already highly vulnerable to infections due to their underlying cancer disease and generally immunosuppressed state, which implies greater risk of serious virus complications, including admission to ICU or even death.
In some Italian and European cities, in fact, the media reported numerous reduction of medical or surgical treatment for neoplasms to prioritize COVID-19 seriously ill patients [23]. During COVID-19 pandemic, head and neck malignancies represent a particularly complicated challenge to be faced by the head and neck surgeon. Literature studies richly report that such malignancies of the head and neck district (tumours of the larynx, advanced tumours of the nasopharynx, base tongue and more widely of the oral cavity) can produce serious respiratory difficulties when left untreated [24]. This issue is particularly relevant for patients affected by laryngeal carcinomas with advanced-stage disease (stage III or IV), which represent 60% of the cases coming to our attention. Given the unique physiological function of the larynx, there are numerous common symptoms that could favour further intervention for laryngeal carcinoma, such as hoarseness, dysphonia, swallowing and dyspnoea [25]. Dyspnoea is indeed present in all the most serious cases of COVID-19 patients. For this reason, early diagnosis and urgent surgical treatment is mandatory not only to guarantee the highest 5-year survival rate but also because a COVID-19 infection in such patients could be fatal in very short time.
At the INT-IRCCS "Fondazione G. Pascale", during the Covid-19 outbreak (21 February-21 Maggio 2020) there has not been a reduction in the treatment of malignant head & neck neoplasms, with particular attention to laryngeal tumors (open surgery, endoscopic LASER) and advanced tumours of the base tongue and oral cavity. Transoral robotic surgery (TORS) has not been suspended, also because a review of the literature has revealed that in selected cases TORS could reduce hospitalization times. All respiratory protection procedures have been adopted and particular attention has been paid to cleaning the robot and the console [26].
One hundred-twenty nine (129) major surgical procedures for head-neck malignancies were performed; among these, 7 total laryngectomies and bilateral neck dissection, 22 partial laser laryngectomies, 6 emergency tracheotomies, 38 major oral surgery interventions, 14 TORS procedures. Only surgical procedures in which the aerodigestive tract was not involved (i.e. parotidectomy), were not subject to the operating room COVID protocol
Furthermore, the head-neck surgeon have been playing another crucial role in this pandemic emergency phase.
In fact, ICU patients undergoing prolonged intubation often require safer airway management of the airways, so in these cases it was necessary to perform a surgical tracheotomy which, if performed in the first 7 days after orotracheal intubation, it is associated with a reduction in the duration of mechanical ventilation and in ICU stay, as well as with the mortality rate [27]. All such procedures require a very high level of containment and are performed under general anaesthesia rather than in sedated patient, given that during the direct access to the trachea there is a large production of droplets from the stoma [28].
Finally H&N medics contributed to the identification of paucymptomatic patients, whose symptoms were mainly anosmia and ageusia [29].
Abdominal Surgical Oncology During Covid-19 Pandemic
Surgical oncology at the INT Fond Pascale has not been stopped by the COVID-19 pandemic but prioritization has been necessarily taken into account to face the need for reduced resources and modified admission and management strategies. Being a potential Covid free hospital, in accordance with a shared strategy, all the Abdominal Surgical Oncology Units tried to identify uniform approaches to minimize the impact on quality and timing of surgery for patients enlisted for elective treatment [30]. Screening of patients for Covid 19 has been widely adopted to identify suspect or positive cases in order to postpone surgery and maintain the safety of both admitted patients and professionals.
Telemedicine, smart-working and web-based multidisciplinary meeting have been promptly adopted to guarantee social distancing. Surgical wards have been remodulated reducing the number of beds for rooms, relatives’ visiting hours have been abolished and daily telephone call with contact persons for each patient have been guaranteed. Rotation and workload have been limited having no more than two doctors working in the ward; also nurses have entered a rotation system to reduce the risk of infections.
Surgical approach
Minimally invasive surgery, both robotic and laparoscopic, has been conducted with a high safety profile by the use of the new insufflation systems, such as AirSeal® iFS (CONMED, USA): it offers continuous smoke evacuations trough an Ultra Low Penetrating Air (ULPA) Filter allowing the capturing of particles > 0.01 µm (CoV-2 virus has a 0.06–0.14 size) [31, 32]. Moreover, this new type of 3 way insufflators keep the abdominal pressure low and has an integrated active smoke evacuation mode which prevents the risk of aerosol SARS-CoV2 transmission. Extensive use of adequate DPI for both surgeons and nurses has been guaranteed [33].
Timing and delay of surgery
In general any delay of surgical approach in abdominal cancer patients could have an impact on survival: despite this a prioritization programme should consider not to delay patients who
-
have completed neoadjuvant approaches
-
have highly biological aggressive tumours
-
do not have alternative strategies for their tumors
Specific sites management
Colorectal cancer
Prioritisation of cases has followed fully shared decisions by the multidisciplinary team taking into account the experience of other centers in Italy [34]. Patients with nearly obstructing or bleeding colonic cancers have received upfront surgery within the expected 30 days from the diagnosis; a similar approach has been guaranteed for patients with complicated high and low rectal cancers. Stoma formation has been selectively adopted to reduce postoperative complications in high risk patients. Also patients with rectal cancers with poor or absent response to neoadjuvant treatment have been operated on. Surgical approach for locally advanced rectal cancer with major or complete response after neoadjuvant treatment has been delayed.
Polyps, asymptomatic carcinoids and prophylactic surgery for hereditary diseases have been postponed. Continuation of neoadjuvant chemotherapy has been planned for those patients with locally advanced colon and rectal cancers within dedicated protocols. in order to delay progression of disease awaiting surgery. Short course radiotherapy has also been considered for early distal rectal cancer, mainly in elderly patients.
Endoscopic stenting for obstructing tumors has also been adopted as a “bridge to surgery” in patients with high anestesiological risk.
Esophageal Cancer
For all hystological types, patients with stage 1 disease have been postponed: stage II and III have been proposed for neoadjuvant therapy. Patients with stage IV disease have been entered in integrated treatment pathways or palliated for symptoms and complications.
Gastric Cancer
Only early tumors have been postponed. Patients with locally advanced diseases have been discussed for neaodjuvant approach that is a standard for many clinical situations. Neoadjuvant chemotherapy has been continued in those with minimal toxicity to delay surgery.
Pancreatic cancer
Neoadjuvant chemotherapy has been identified has the best approach for all uncomplicated cases. Surgical approach has been guaranteed to patients already treated with chemo-chemoradiation. Endoscopic stenting and gastrojejunal bypass have been offered to symptomatic patients.
Liver tumours
Surgical approach, both with minor or major resections has been guaranteed in patients with liver metastases already treated with chemotherapy in a neoadjuvant approach. Careful selection of patients has allowed to postpone those at high risk of postoperative complications. Local ablation for both primary and metastatic tumors has been regularly performed.
Retroperitoneal sarcomas
Surgical approach, also in case of extended multivisceral resections, has been guaranteed in patients with localised and resectable tumors with minimal delay. Biologically aggressive tumors have been entered in integrated treatment pathways.
Peritoneal neoplasms
Being peritonectomy followed by hypertermic peritoneal chemotherapy a very aggressive procedure, patients with primary and metastatic peritoneal tumors have been postponed.
COVID-19 and Radiotherapy
Radiotherapy is a life-saving treatment and must be guaranteed for cancer patients for whom it is indicated, as requested by several oncological Scientific Societies [35]. It is estimated that 60% of cancer patients should include radiation therapy as part of the treatment.
Radiation therapy plays an important role in cancer patients as neoadjuvant treatment before surgery, adjuvant therapy after a primary treatment of surgery, concomitant to other therapies for synergistic enhancement of systemic treatments and exclusive treatment. In these cases, failure to administer radiotherapy adversely affects local control and overall patients’ survival. Finally, in patients with bone or brain metastases, bone marrow compression and mediastinal disorders palliative radiotherapy significantly improves pain control and quality of life.
During COVID-19 outbreak radiation therapy departments could represent a site of exposure for patients and operators because radiotherapy usually involves daily treatment for days or weeks in a closed environment (many radiotherapy centers are situated in basements). In this respect, one of the main critical problems was the management of patients’ flow and their caregivers who access radiotherapy facilities. For this reason, it was necessary to develop specific protocols and protective measures to prevent the spread of COVID-19 during radiation procedures and reduce the overcrowding of facilities and the risk of infection among fragile and vulnerable patients and staff [36, 37].
All the clinical activity, comprising CT-simulation, were re-scheduled in order to reduce the risk of contagion for both patients and staff. During emergency phase 1, doctors, physicists and administrative staff work in two shifts with rotation assignments and all activities that did not require on-site presence (such as phone calls and physicists planning) were carried out via telemedicine. In particular, it was scheduled the presence on-site of one medical physicist supported by colleagues in remote working. Live staff meetings were no longer performed and staff workstations were located in different areas to allow social distancing.
Adequate interval time between CT-simulation and start of the radiation therapy was guaranteed with no further delay or extended radiotherapy interruption. As results of our strategies, there was no reduction in terms of number of patients treated during COVID-19 outbreak, but there was a reduction in the treatment waiting list. In the first trimester of 2020, 614 treatments were performed in comparison to the 598 treatments performed in the first trimester of 2019.
Figure 3 shows the number of treatments delivered in the first trimester of the two years (2019 and 2020) stratified by pathology. Hypofractionated regimens have been favored [38, 39]. Moreover, collaboration with Ascalesi Hospital in Naples, have favored the treatment of a greater number of patients with an increased number of breast cancer and bone metastasis treated in 2020 compared to 2019.
In general, treatments that included neoadjuvant hormonal therapy were postponed, whereas radiation therapy was ensured for patients with in situ cancers and for adjuvant or concomitant radiation therapy candidates.
Figure 4 and 5 compare the activities carried out in the first three months of 2019 and 2020 and in March 2019 and 2020, respectively. As observed in Fig. 2, there was a slight reduction of first clinical evaluation in the first trimester of 2020 compared to 2019. This was due to the postponement of radiotherapy access for patients eligible to neoadjuvant systemic treatment. Instead, thanks to collaboration with Ascalesi Hospital, every patient candidated to a radiation treatment that could not be postponed was treated. Figure 3 shows a reduction of activities in March 2020 compared to 2019, as consequence of Italian lockdown for COVID-19 outbreak emergency measures introduced by the government on March 9.
This reduction, has affected: the first clinical evaluation because, following multidisciplinary evaluation, radiation treatment was delayed for a few months in patients for whom a hormone neoadjuvant therapy was possible; simulation CT because only patients who must start quickly radiation treatment were simulated, and the number of follow-ups. Furthermore, in March 2020 we performed 214 treatments compared to the 207 ones in March 2019.
With regard to follow-up visits, further clarification is required respect to graphic shown in Fig. 5. Radiation oncologists, using telemedicine (telephone calls, app and emails), carried out
340 follow-up visits. Thirty-three outpatient visits were performed in the first week of March 2020, then, after government lockdown law, each patient was telematically guided to share diagnostic tests with the radiation oncologists. Many prostate patients’ follow-up were performed by our ProstateRadioTherapy App, which has been used as routine clinical practice for several years. The app collects and stores biochemical parameters, genitourinary and gastrointestinal toxicity, sexual activity and quality of life questionnaire data entered into the database. Thanks to the app, the radiotherapy staff constantly follows more than 100 patients with prostate cancer and, during the COVID-19 emergency, has proven to be an important tool for the management of these patients. Therefore, in March 2019 of the total 404 radiotherapy follow-ups 279 (69%) were carried out in the Department, while in March 2020 of the total 340 follow-ups only 33 access (9.7%) were on-site. These data show that telemedicine was applied in 90.3% of cases with a consequent drastic reduction in patients' access to the facility.
Of note, some patients were unable to perform clinical exams because of Covid-19 emergency. As consequence, it was recorded a reduction of about 16% of total follow-up visits in March 2020 compared to the March 2019 (Fig. 6).
In the so-called "emergency phase 2" which will begin at the end of the lockdown, the staff will be scheduled in two 8-hour work shifts, with approximately 3 hours of overlap used for telemedicine activities. In this way all the activities will be guaranteed for 12 hours a day ensuring social distancing
Diagnostic procedures
• Diagnostic imaging
The INT-Pascale Diagnostic Imaging units has contributed to identify COVID-19 patients and to evaluate the lung parenchyma involvement. Although our Institute is not a COVID-19 hospital (not dedicated to hospitalization of SARS-CoV-2 infected patients) all diagnostic units have been involved in identifying potential COVID-19 patients for their isolation and subsequent transfer to COVID-19 hospitals. All hospitalized patients with suspicion of COVID-19 for symptoms of acute respiratory infection, while waiting for the swab collection and PCR analysis, have been assisted in hospital ward and subjected to chest X-ray at patient's bed to evaluate the involvement of the lung parenchyma. Chest X-ray examination, although not offering highly specific findings, provides a first overview of the patient and may direct differential diagnosis to other possible causes of pulmonary parenchymal involvement other than Covid-19 infection [40]. Bandirali et al. at the Codogno Hospital, where the Italian COVID-19 epidemic was recognized, were able to identify chest x-rays abnormalities highly suspicious for COVID-19 pneumonia in 100 of 170 (59%) patients [40]. Involvement was bilateral in all cases: in 54% of patients the involvement was symmetrical. Furthermore, chest X-ray at the patient's bed is a valid tool for the evolutionary monitoring of pneumonia in hospitalized patients and in intensive care [41, 42]. Following X-ray, COVID-19 suspicious cases have been subjected to the nucleic acid amplification test of the respiratory tract or blood specimens using reverse transcription real-time polymerase chain reaction test (RT-PCR). In case of positive RT-PCR, patients have been transferred to regional infectious disease centers dedicated to COVID-19 management. Since the X-ray suspicion of COVID-19 infection, patients have been isolated in sub-intensive rooms and monitored with the appropriate diagnostic and laboratory test, waiting for the PCR results and eventual transfer to COVID-19 hospitals.
In this context, recent results have revealed the efficiency of some imaging methods in the management of COVID-19 disease. The chest ultrasound (POCUS - Point-Of-Care UltraSound) can be performed by the intensivists at the patient's bed and represent a valid monitoring tool to evaluate the effectiveness of the prono-supination maneuvers [42–44]. POCUS can reduce the use of diagnostic imaging resources, risk of contagion for personnel, and sanification time. Moreover, it helps in POC decision for critically ill patients. On the other hand, the ultrasound scan itself requires prolonged contact between the operator and the patient, and has other contraindications, including dependence on operators [42–44]. Computed tomography (CT) examination has been used extensively in China and now worldwide to evaluate the grade and the extension of the viral pneumonia by COVID-19 especially in the follow-up [45–47], also supported by Artificial Intelligence algorithms [48, 49]. Bilateral distribution of ground-glass opacities, with or without consolidation, in posterior and peripheral lungs was initially described as a characteristic feature of COVID-19 [48, 49]. However, several radiological organizations do not recommend CT as primary screening tool for COVID-19 [50–54]. Moreover, safely using CT to study COVID-19 patients is logistically challenging and can overwhelm available resources. Even with proper cleaning protocols, healthcare professionals and CT scanners could become vectors of infection to other vulnerable patients who require CT imaging.
• Diagnostic procedures (Laboratory Medicine)
The Laboratory Medicine Unite of the INT Pascale has been involved since the beginning of the epidemic in the identification of the COVID-19 patients as well as on the early SARS-CoV-2 exposed health workers. The promptly organized COVID-19 crisis unit of the INT, in fact, under the General Director (Dr Attilio Bianchi) solicitation established a program of health surveillance for all patients as well as healthcare workers with travel, exposure or symptoms history suggestive for infection with SARS-CoV-2. Moreover, molecular methods were selected as a gold standard and immunology tests (i.e. serology and rapid antigen tests) recognized as supplementary diagnostic tools [55]. The Laboratory Medicine personnel (medical director), first of all, identified and implemented the biosafety conditions recommended by World Health Organization’s interim guidance [56]. A validated internal protocol including pre-analytical, analytical and post-analytical phases (from sample transportation to elaboration of medical reports) was derived from it.
The diagnostic workflow applied at the INT Pascale included both:
Molecular testing, as recommended by the World Health Organization, has been used as reference method for the identification of SARS-CoV-2 infectious cases [57]. Nucleic acids extraction and subsequent Real-time PCR detection of SARS-CoV-2 RNA from nasopharyngeal swabs were performed [58]. The Charité algorithm (Berlin, Germany) worked out by Christian Drosten and colleagues, based on Real-time PCR detection of E and RdRp genes was used as a reference method [59]. Molecular testing found application primarily in early stages of disease and in detecting asymptomatic carriers.
Rapid immunochromatographic assays, used as an additional diagnostic procedure, have shown the advantage of rapid results times and low cost detection. However, they were likely to suffer from poor sensitivity and limited specificity making them more useful in monitoring positive subjects than in the initial diagnosis.
According to good microbiological practice and procedure, initial processing (before virus inactivation) of specimens from cases with suspected or confirmed COVID-19 infection has taken place in a validated biological safety cabinet. Either propagative or non-propagative diagnostic laboratory work has been conducted in a laboratory area following biosafety standards. Only staff trained in the relevant technical and safety procedures has been admitted in handling and processing hazardous specimens, according to internal protocol. In particular, two laboratory technicians were provided with appropriated personal protective equipment and assigned to these activities. Management of assays interpretation, results and medical reports was committed to a single healthcare worker, in order to standardize the post-analytical phase. Patients’ results were made available promptly to wards by means of “order entry” data visualization, whilst reports relative to hospital personnel were transmitted only to the Medical Director of the surveillance office.
All the efforts of the staff involved in COVID-19 diagnostic procedure have been directed to guarantee an adequate turnaround time, in order to furnish results in a shorter time as possible. As a matter of fact, the element “time” has been crucial to subject promptly to home quarantine personnel identified as positive or move to reference hospitals affected patients.
• Diagnostic procedures (Pathology Unit)
The Pathology Unit, involved in all extemporaneous exams on fresh samples diagnostic procedures, in particular tailoring radicality in demolitive surgery, has promptly chosen and implemented special and extraordinary precautions for management and handling of biological samples. The SARS-Cov2 virus has been identified mostly in tissues and biomaterials of lung origin, but, although more rarely, in other biomaterials, including blood [60]. Therefore, in the Pathology Unit, given that the SARS-CoV-2 can be present in all surgical and cytological biomaterials, fresh or inadequately fixed, all biological samples have always been considered potentially infected and consequently all operators have been equipped with adequate personal safety devices (PSD).
The handling of biological samples regards in particular the "acceptance" and the "processing" steps of tissue and cytological samples. For the acceptance it must be distinguished whether the samples are coming from the hospital operating theatre or from second opinion outpatients: i) for surgical and cytological samples, in particular pulmonary samples, access to the pathology laboratories of surgical operators, equipped with the PSDs, and the delivery of the samples to selected, dedicated technician was provided at set times. ii) in front of the laboratories of the Pathological Unit, a Triage facility was set up to monitor the temperature of the patients who, also equipped with a mask and at a safe distance, arrive for the request of a "second opinion" on biomaterials already prepared. All biomaterials that arrived in the laboratories were always accompanied by a request containing the clinical information relating to the SARS-Cov-2 infection.
For the "Processing" of biological samples they have been all considered at microbiological risk. Samples have been fixed immediately in 10% buffered formalin for at least 24 h at a temperature between 25 °C and 37 °C, following the recommendations of the SIAPEC-IACP (Società Italiana di Anatomia Patologica e Citologia Diagnostica-Divisione Italiana della International Academy of Pathology) [61]. This procedure, even if it favors the containment of the biological risk over the chemical one, promoting the use of formalin, allows to inactivate almost all the viral particles in the tissues. The subsequent handling of the samples was performed under hoods with biosafety characteristics to contain the biological risk.
As for intraoperative procedures, which require the handling of fresh tissue samples, it is not recommended for SARS-CoV-2 positive or suspect patients, especially for lung lesions [62]. In other cases, the samples have been immediately processed with the appropriate precautions and the expected PSDs. However, diagnostic imaging strategies were implemented during the pre-operative phase, to minimize the need for intraoperative examinations.
{kind=link}