CD79B and PIM1 mutations are independently related to POD12 following R-CHOP treatment
Total 32 hotspot driver genes were examined using next-generation sequencing in 145 newly diagnosed patients with DLBCL. All of these genes were mutated in 91.72% patients (133/145) with a median number of 4 (0-24), including single nucleotide variants, frameshift mutations, insertions, and deletions. SNPs were filtered according to the defined criteria. The frequency of CD79B (42.86% vs 9.38%, p = 0.000) and PIM1 mutations (38.78% vs 17.71%, p = 0.005) showed a significant increase in patients with POD12 (n=49) (Figure 1), but no difference was found in median number of mutations (5 vs. 4, p = 0.287). The POD12 patients had very poor survival and almost all of them presented systemic relapse except for three patients involving central nervous system. When the associations of gender, age, ECOG score, Ann Arbor stage, LDH level, the number of extranodal involvement, IPI score, COO, DE, and positive p53 protein with POD12 were evaluated, univariate analysis displayed an obvious correlation with Ann Arbor stage (p = 0.019), LDH level (p = 0.001), IPI score (p = 0.014), and DE (p = 0.001) (Table 1). Multivariate analysis, including Ann Arbor stage, LDH level, DE, and gene mutations of CD79B and PIM1, revealed that LDH level (OR = 2.990, p = 0.018), CD79B (OR = 5.970, p = 0.001), and PIM1 mutations (OR = 3.021, p = 0.026) were independently correlated with POD12.
CD79B and PIM1 mutations are associated with complex genetic events and unfavorable prognosis
Complex genetic events were seen involving in CD79B and PIM1 mutations (Figure 2a). There were 36 mutational sites occurring in 30 patients with CD79B mutations, including 8 in the Ig-like V type domain, 5 in the transmembrane domain, and 23 in the immunoreceptor tyrosine-based activation motif (ITAM). A prominent site was identified at the Y196 of ITAM in 63.3% (19/30) of patients. Moreover, 25 gene alterations were observed to accompany with CD79B mutations, only PIM1 (14/36, p = 0.002) and MYD88 L265P (11/16, p = 0.000) mutations having significant correlation. 105 mutational sites of PIM1 were seen in 36 patients, a majority of which occurred in the kinase domain with V177 (4/36, 11.1%), S188 (6/36, 16.7%) and E226 (6/36, 16.7%) having high frequency involvement. There were 30 gene alterations accompanying with PIM1 aberrations, including IRF4 (9/14, p = 0.001) and MYD88L265P (10/16, p = 0.000) alterations having obvious correlation.
By analyzing clinicopathological features, CD79B mutations were significantly associated with DE (p=0.001) and non-GCB subtype (p=0.030), and PIM1 mutations were statistically relevant to DE (p=0.049) and advance stage (p=0.023) (Supplementary Table 2). Patients with CD79B mutations manifested poorer PFS and OS than wild-type patients, while patients with PIM1 mutations presented poorer PFS, but not OS (Figure 2b). In a larger cohort [17], both CD79B- and PIM1-mutant patients were found to have worse survival than those with wild-type genes (Figure 2c). These data indicate that CD79B and PIM1 mutations are associated with complex genetic events and unfavorable prognosis.
A robust predictive model for POD12 is created by incorporating the variables CD79B mutations, PIM1 mutations, and LDH levels
We established a new genetic predictive model for POD12 after integrating LDH levels (OR = 2.990, p = 0.018), CD79B mutations (OR = 5.970, p = 0.001), and PIM1 mutations (OR = 3.021, p = 0.026), which were independently related to POD12. In this genetic predictive model, LDH levels and PIM1 mutations were defined as a score of 1, and CD79B mutations was assigned as a score of 2 based on their OR value. The analysis of AUROC (0.771, 95% CI: 0.689-0.853) demonstrated the model to have a good performance. With the highest Youden's index of 0.4052, scores of 2-4 were recommended to distinguish low- and high-risk patients of POD12 with a sensitivity of 55.10% and a specificity of 85.42%. The incidence of POD12 was significantly increased in patients with scores of 2-4 compared with those with scoring 0-1 (21.15% vs 65.85%, p= 0.000), who also displayed poorer PFS and OS (Figure 3a and 3b). The genetic predictive model was successfully validated in a cohort of 84 cases and in another larger cohort of 1001 patients [17] (Figure 3c, and 3d). The cohort of 84 patients was enrolled in our center and exhibited similar features with the cohort of 145 cases. The larger cohort was derived from Reddy. B et al study [17], which almost addressed these characteristics above mentioned except for positive p53 protein and special site of extranodal involvement. In comparison with the other two cohorts, it had higher proportion of the elderly (56.6% vs 27.6% vs 20.2%), IPI score 3-5 (44.3% vs 25.5% vs 23.8%), and lower frequency of CD79B mutation (4.7% vs 20.7% vs 20.2%) (Supplementary Table 1). The discrepancy may come from selection and/or ethnic deviation. However, patients with high-risk POD12 showed very poor survival in the larger cohort (p=0.000) (Figure 3d).
Our modeling was further compared with traditional IPI score and new molecular subtypes, MCD and Cluster 5, on the power for predicting POD12. The MCD subtype is defined as a co-occurrence of CD79B and MYD88L265P mutations [18] and Cluster 5 is a genetic signature having frequent mutations in CD79B, MYD88 L265P, and PIM1 [16]. The result showed that the value of this genetic model in predicting POD12 is superior to conventional IPI score and MCD subtype (Figure 3e). The association of Cluster 5 with POD12 was not found (12/64, p=0.576) by analyzing the data from Chapuy. B et al study [16], either. Collectedly, we created a predictive model for POD12 with a powerful performance by incorporating the variables CD79B mutations, PIM1 mutations, and LDH levels.
CD79B and PIM1 mutations indicate better response to BTK and pan-PIM kinase Inhibitors, and BCL2 inhibitor enhances their apoptosis-inducing effects in cells with DE
A novel treatment was evaluated based on our predictive model. By sequencing a panel of 32 hotspot driver genes in 5 DLBCL cell lines, only Val cells had a CD79B mutation in the ITAM domain (T212M), and OCI-Ly8 cells had PIM1 mutations in the kinase domain (S188N and L284F), which were both accompanied by mutations in MYC, BCL2, FOXO1, and CREBBP. Val and OCI-Ly8 cell lines were used to test the effects of CD79B and PIM1 mutations on DLBCL cells sensitivity to BTK inhibitor ibrutinib and pan-PIM kinase inhibitor AZD 1208. Cell proliferation assay was carried out to determine experimental doses of ibrutinib and AZD1208 (Figure 4a). We found that CD79B-mutant Val cells were more susceptible to 10 µM ibrutinib-induced growth inhibition and apoptosis when compared with CD79B-wildtype OCI-Ly8 cells (p < 0.01); PIM1-mutant OCI-Ly8 cells also presented a better response to 40 µM AZD 1208 than PIM1-wildtype Val cells (p < 0.01) (Figure 4b, 4c, and 4d). The significance of PIM1 mutations was further confirmed in xenograft mouse models. After AZD 1208 was given daily according to the protocol, tumor growth was significantly suppressed in OCI-Ly8 xenograft mice when compared with Val xenografts (Figure 5a). These results suggest that CD79B and PIM1 mutations make DLBCL cells sensitive to BTK and pan-PIM kinase inhibitors.
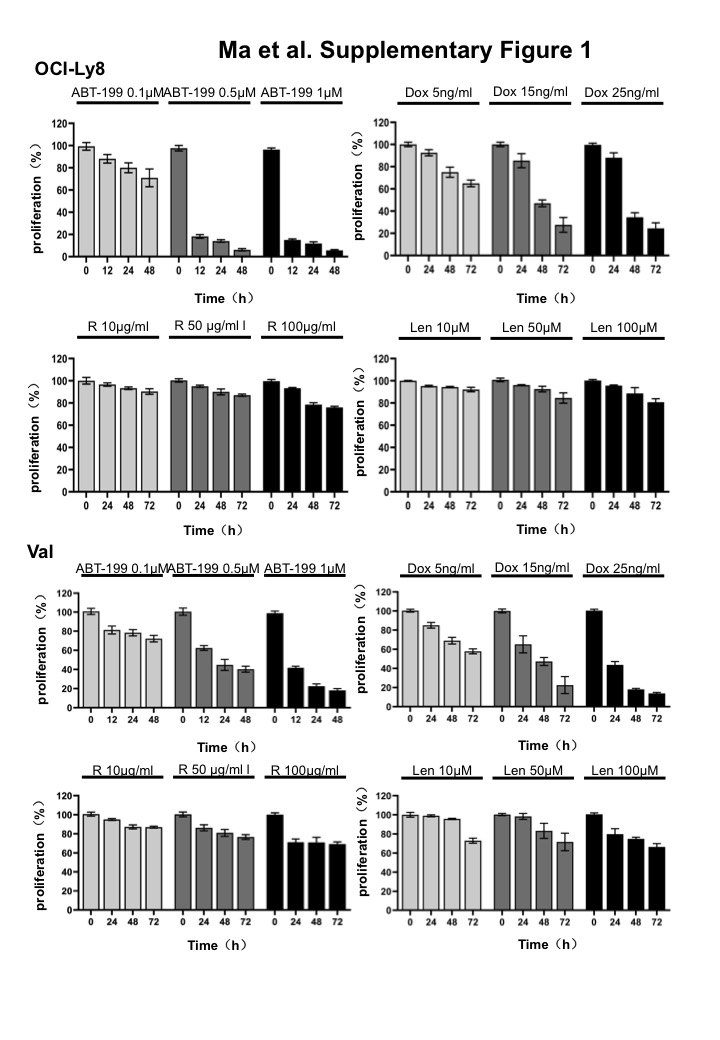
Next, we determined the action mechanisms of the two inhibitors by Western blot. A gradual increase of cytoplasmic IκB and a reduction of nuclear p65 were found after ibrutinib treatment for 24-72 h, while phosphorylated-CDC25A was decreased following AZD 1208 treatment for 24-72 h (Figure 5b). Both c-MYC and BCL2 proteins were found to present in Val and OCI-Ly8 cells. However, c-MYC expression, but not BCL2 expression, was significantly reduced by ibrutinib and AZD1208 (Figure 5c). Therefore, BCL2 inhibitor venetoclax was added to enhance the effectiveness of ibrutinib and AZD 1208. We picked 0.1µM venetoclax for experiment based on the results of cell proliferation assay (Supplementary Figure 1). Encouragingly, venetoclax did show a prominent synergistic effect when combined with ibrutinib and AZD 1208, even though it alone did not produce obvious apoptosis (Figure 6a). The observed effect of venetoclax should be attributed to its inhibition of BCL2 function, since BCL2 levels were not affected (Figure 6b). The combinatorial effect of other key agents for DLBCL therapy, including rituximab, doxorubicin, and lenalidomide, were also examined with ibrutinib and AZD 1208. Their doses in in vitro assay were also chosen based on the results of cell proliferation assay (Supplementary Figure 1). The results showed that 100 µg/ml rituximab, 15 ng/ml doxorubicin, and 50 µM lenalidomide only produced rather limited synergistic action of apoptosis with ibrutinib and AZD 1208 (Figure 6a). Although some of them exerted inhibitory effects on BCL-XL and MCL1, they have no effect on BCL2 expression (Figure 6b), suggesting the importance of blocking BCL2 in promoting apoptosis of mutant cell with DE.
{kind=link}