The First Affiliated Hospital of Zhejiang University School of Medicine (Zhejiang University First Hospital for short), as a designated hospital for patients with severe novel coronavirus pneumonia in Zhejiang Province, admitted and treated a total of 105 confirmed cases (including 78 cases of severe and critical cases) and excluded 183 suspected cases, without any cases of COVID-19 among medical staff and patients in the hospital. Simultaneously, a medical team was sent to take over the new coronavirus pneumonia ward in several hospitals in Wuhan, and at the same time completed the rescue and treatment tasks, the medical staff also achieved zero infection. The prevention and control of hospital-acquired infections have played a key role in the prevention and control of this COVID-19 epidemic, and we, therefore, hope to share our experience of diagnosis and treatment with other countries in order to combat this global epidemic.
SARS-CoV-2 is a newly discovered virus for which there is currently no effective specific vaccine for its infection, therefore isolation of infected persons and prevention and control of at-risk populations is of great importance. Identification of COVID-19 in patients with chronic infective wound presenting with nonspecific symptoms is challenging and difficult, especially in non-outbreak areas, where early clinical and imaging presentation of COVID-19 was not characteristic(29). At the same time, nearly 73% of patients infected with SARS-CoV-2 are men, as well as old age, diabetes and lung disease are also independent risk factors, thereby the control of such groups is also of particular importance(3, 30).
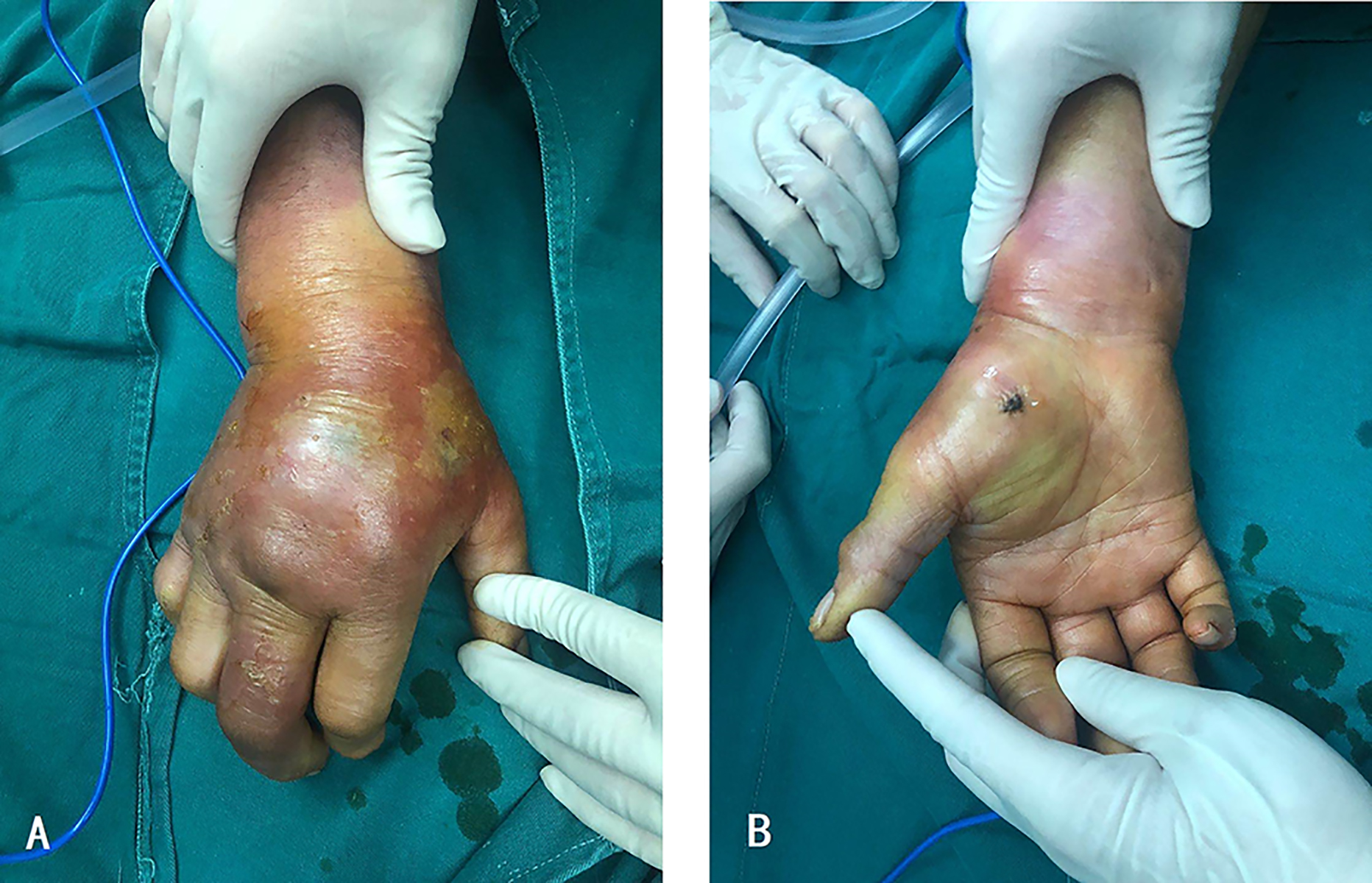
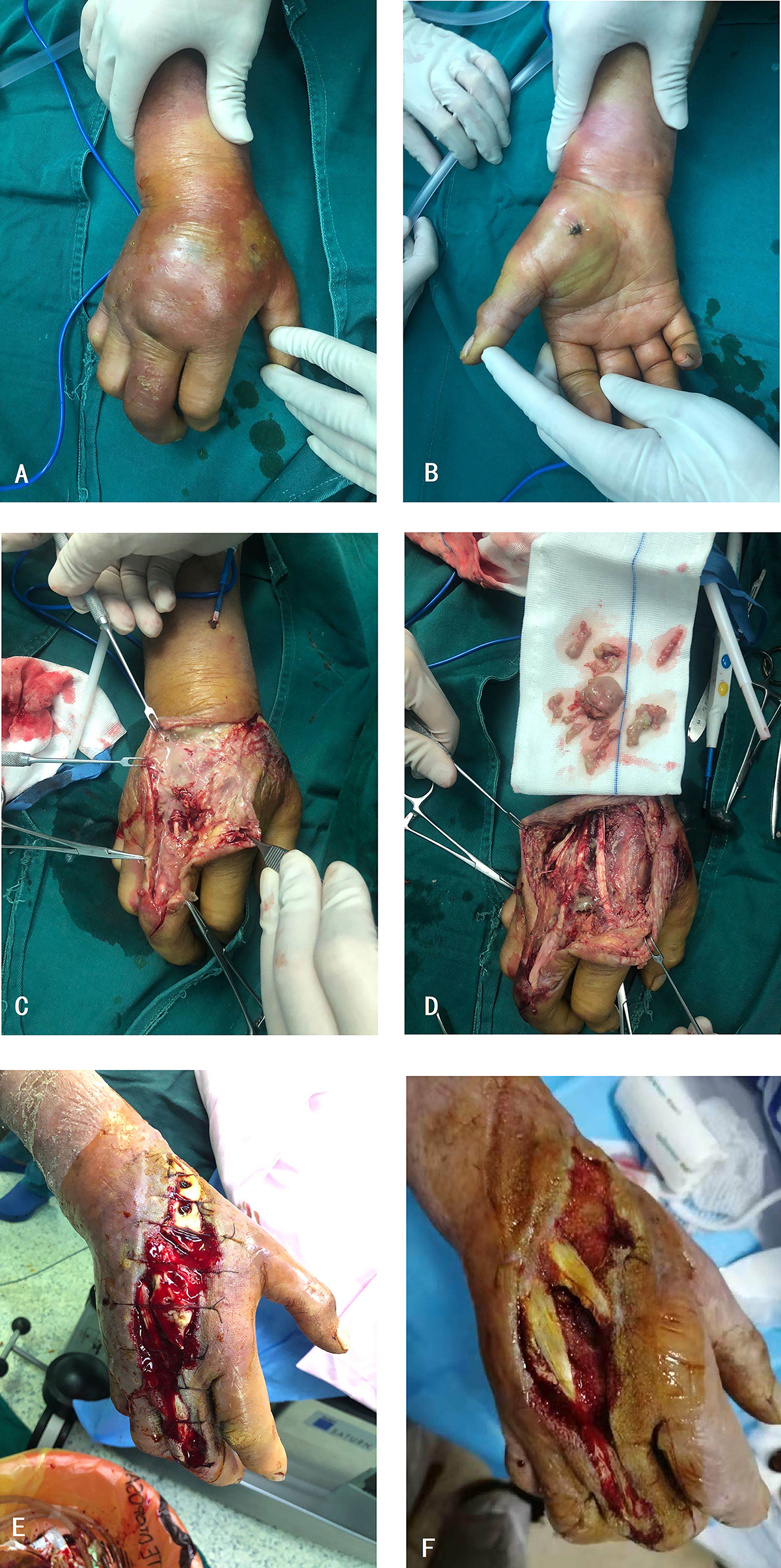
In a survey of chronic wound patients documented in China between 2018 and 2019, it was found that 76.74% of patients over 50 years of age had comorbid underlying diseases, of which 78.25% had comorbid underlying diseases, and the top four were diabetes, cardiovascular disease, hypertension and respiratory disease(31, 32). Our study also shows that patients with chronic infective wound are predominantly older men with multiple underlying conditions, who happen to be at high risk for coronavirus infection. In addition, chronic wound often requires specialized clinical care due to the susceptibility of the lesion and the prolonged changes in the disease, otherwise their simple superficial infections will worsen, causing systemic infections, amputations and even death(33). In our study, as we reviewed patients' medical records, we found that many patients were unable to seek medical attention in time during the epidemic, which resulted in delaying the best opportunity for treatment and causing the deterioration of the wound to require surgical treatment, therefore, it is of great importance to arouse people's attention to wound care during the epidemic. Just for instance, an elderly male (66 years old) was stabbed with a brick in his right interosseous after a sudden fall. Without sufficient medical support, only a simple hemostatic bandage was performed, and 20 days later, the patient developed a severe infection in his right interosseous region along with significant hand swelling and osteofascial ventricular syndrome [Fig S1]. Eventually he underwent chronic ulcer repair and decompression of compartment hypertension, which will be described later. It can be seen that that appropriate antibiotic therapy and timely surgical debridement or drainage are crucial for the control of the disease in these patients, whereas on the other hand, it leads to the inevitable need for regular hospital visits, which increases the risk of COVID-19 infection due to transportation and in-hospital treatment. Therefore balancing the control of wound progression and the reduction of the risk of coronavirus infectious during COVID-19 epidemic is a particular challenge for chronic wound patients.
Based on the WHO recommendations for the clinical management of COVID-19, the Novel Coronavirus Pneumonia Protocol (7th Edition) issued in China, and our treatment experience in the First Affiliated Hospital, College of Medicine, Zhejiang University, for all patients with chronic wound we recommend the application of APPs that used to Personal Health Status Identification(34), such as the implementation of the Green Health Code in China, which plays an important role in the identification of the epidemiological history of patients who require multiple trips to hospitals or other place, along with the full integration of telemedicine and nosocomial infection control during the COVID epidemic to reduce patient risk of infection(35). First, patients are advised to seek medical help on the Internet, then doctors learn the patient's epidemiological history, symptomatic signs, and other information online, triage the patient, and, on the basis of stabilization, if possible, advise the patient to self-treatment, guided therapy or nearest treatment, to reduce the risk of exposure during transportation(36). When patients have to go to the hospital, the information obtained is used to classify patients into low-risk and middle-to-high-risk patients which applies to implement dual-channel triage, and meanwhile control the waiting spacing, and reconfirm the patient's medical history and other information at the triage desk, to reduce the risk of infection in outpatients. Besides, the hospital must strengthen the education of infection prevention knowledge for all personnel, even for cleaning personnel, and the storage of protective materials and indoor ventilation measures. In the wards, we suggest that hospitals with the conditions can set up a special branch to receive infected or suspected patients, such as our hospital has a special area of Zhijiang hospital, otherwise, emergency isolation wards should be set up within the ward for medium to high-risk patients with COVID-19 and general wards. In addition, the wards can be divided into contaminated areas, buffer zones and clean-up areas, and, if possible, medical equipment and responsible medical personnel can be fixed in each bed to achieve more precise protection. Chaperones in the ward should also avoid excesses, and educate the patients and their relatives on infection prevention and control. In the case of surgical patients(36-38), our recommendation is to avoid surgery during a pandemic as much as possible and, in the case of limited duration surgery, to avoid the risk of aerosol transmission of the virus by selecting a negative pressure operating room or at least an operating room with independent ventilation. Furthermore, avoid invasive airway manipulation as much as possible, e.g. nerve block anaesthesia for anaesthetic measures, thus reduce the risk of respiratory tract infection.
In the course of medical treatment, it is not only necessary to pay attention to contagion among patients, but also to be alert to medical personnel as a source of contagion, who is also the backbone of the battle against the epidemic, therefore, social isolation and personal protection of medical personnel should also be paid attention(35). When physicians share a room with COVID-19 patients, their chances of infection are greatly increased, especially when performing invasive procedures, and then they may become new source of infection to their intimates(39, 40). A single surgical procedure can trigger transmission of the virus, and when a clinician is faced with a chronic trauma patient with COVID-19, multiple dressing changes inevitably increase the risk of COVID-19 transmission. Thus, doctors should not only take care to keep themselves at a distance from the patient's airway and isolated from the patient's body fluids, but should also practice social distance between their colleagues. Meanwhile, given the enormous medical stress caused by the COVID-19 epidemic, it is also important for health care personnels to choose appropriate ways to release stress to avoid serious mental illness(41).
Meanwhile in this study,we found that among three types of wounds, patients with other types of soft tissue infections were the most common, thus these patients were the most easily encountered in clinical work during the COVID-19 epidemic. The following is gangrene due to vascular occlusion, which is also the type of chronic wound with the longest hospital stay and the most risk factors for COVID-19 as shown in Figure 6. Not only that, but the two types of wound are also slightly similar in clinical presentation, and in our study, most patients presented with lesions of the extremities, with localized swelling, redness, fever of skin and pain manifesting early in the disease. When it comes to the COVID-19, it may perform the same(42, 43).
Therefore, in addition to the above-recommended management requirements for all chronic wound, we suggested that for these two kinds of patients we not only classify them according to the severity of their condition, but also strengthen our comprehension of the epidemiological history and underlying disease status of these patients and stratify the risk of COVID-19 infection(33, 44). Through the implementation of Internet telemedicine and electronic follow-up, as mentioned above, for patients with mild and manageable disease, we would recommend them to take medication and isolate themselves at home, perform appropriate activities and monitor changes in the lesion area. While for patients with thrombotic disease, the detection of INR index is very important, so we suggest that, based on a stable condition, the time interval between visits to the hospital for INR testing can be extended, or using home testing or staggered testing in hospital to reduce the risk of contact transmission and nosocomial COVID-19 infection. In the case of inpatients, after the management of the block by separating hospital district, ward and sector area to reduce the risk of nosocomial infections, the choice of treatment options we recommend are that, on the basis of maintaining the stability of the disease, priority should be given to drug treatment, invasive treatment such as surgery or intervention need to be postponed as far as possible. If the underlying disease is more serious, the patient should first undergo a multidisciplinary consultation to control the comorbidities, and after the comorbidities have been stabilized, the patient can undergo wound treatment, and should be well prepared for repeated treatment. For example, during this outbreak, we received a middle-aged male patient (47 years old) with hypertension, diabetes, and severe heart disease, including dilated cardiomyopathy, heart failure, and coronary heart disease, and was admitted to the hospital for soft tissue infection caused a wood barb wound in his left hand [Fig S2]. COVID-19 infection was ruled out after prehospital screening and the patient was transferred to a general ward. After examining the patient's cardiac function (40% left ventricular diastolic function, moderate stenosis of the left anterior descending branch of the coronary artery, and mild stenosis of the right coronary artery), we invited the cardiology department for a consultation to assess the risk of surgery. Then the patient underwent finger amputation and wound repair [Fig S3]. Since the patients were generally poor which contribute to the unsatisfactory invasive healing, again, we performed 7 times of chronic ulcer clearing and repair procedures after adequate preoperative preparation and patient evaluation [Fig S4]. Finally, the patient was well-covered by the graft wound and was discharged smoothly for home anti-infection, treatment of underlying diseases and regular wound reviewing [Fig S5]. For patients combined with COVID-19 infection, one difference is that attention needs to be paid to the interactions between COVID-19 clinical trial drugs and anti-infection, antiplatelet or other drugs(45). Meanwhile it is also important to prevent these diseases, which may increase the length of hospitalization and the risk of COVID-19 infection, and may make it more difficult for patients with COVID-19 infection to be treated clinically. We, therefore, recommend preoperative and intraoperative prophylactic antibiotic use for all surgical patients. And in the case of bedridden or limited mobility patients, pharmacological prophylaxis should be considered after individual assessment, given their increased risk of thrombosis.
When it comes to trauma-induced chronic wound, as it has an inevitable need for surgical treatment such as debridement, suturing and drainage, we recommend that all such patients undergo screening for COVID-19 like chest CT and nucleic acid testing, and considering that such inpatients require multiple surgeries and are prone to fever during hospitalization, thus a well-developed process is needed, such as timely review of chest-CT and invitations to the infection unit for consultations, etc. For COVID-19-positive or high-risk patients, they should be immediately isolated and operated in the designated negative-pressure operating room, along with disposable surgical items as far as possible, and streamline the required medical staff. Post-operative patients continue to receive isolation therapy and associated trauma care as soon as they return to the ward. Patients who are COVID-19 negative or at low risk should also be seen in a clean area, and surgical masks should be worn to reduce the chance of droplet transmission during the surgery. At the same time, the surgical instruments should be strictly disinfected, packed and transported, and the operators should be as few as possible and wear protective equipment. Strict intraoperative adherence to routine aseptic procedures, with thorough debridement and negative pressure suction, is also important for subsequent wound recovery. Postoperatively, antibiotics can be applied for infection prevention, and regular wound cleaning and replacement of negative pressure suction devices can be performed to promote wound recovery [Fig S6]. After discharge, patients should be followed up electronically, including guidance on wound care and the use of antibiotics, and patients should be asked to change their medications regularly at their nearest clinic, so that they can receive efficient and adequate medical support during the epidemic.
There are still some limitations to this study. Firstly, this center is not the epicenter as Wuhan is, thus, novel coronavirus pneumonia has a smaller infection base in this region, and there is a lack of a richer patient population and a large enough sample size to support the results more reliably, and it is hoped that the findings here will encourage larger cohort studies in other regions or possibly some randomized controlled trials. Secondly, since this is a retrospective study, it is not possible to conduct a prospective study on the probability of COVID-19 infection in all patients with chronic wounds, and it is hoped that this will inspire other researchers to conduct studies on this issue and raise the awareness and treatment of this condition among clinicians and the public.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}