The pathogenic mechanism of COPD remains to be clarified. Viral infections(14) and increased production of autoantibodies.(23, 24) might be contributed to COPD. However, no specific definite virus or immune mechanism has been identified to date. In this study, it was found that LC3 gene expression had no significant difference between COPD group and healthy controls, indicating that the distribution of LC3 is not affected by COPD or smoking. However, p62 gene expression levels of COPD group were significantly higher than those of healthy control groups. The amount of LC3II/l and P62 were both increased in the COPD group, suggesting increased autophagy in the COPD group. Pearson correlation analysis showed that autophagy level and the amounts of CD8+T cells in COPD had a positive correlation.
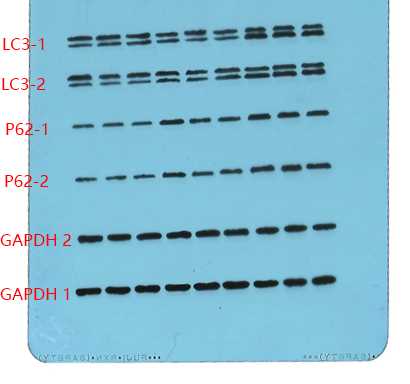
The gene and protein expression levels of LC3 were equally almost the same among the three groups, while the amount of LC3II/I protein were significantly higher in the COPD group compared with the other two groups. LC3 is an autophagic biomarker gene for mammalians and homologue to the yeast Atg8 (autophagy associated gene); It is widely distributed within mammalian cells and generally highly expressed during autophagy.(19, 25) LC3 has two formations, including LC3I and LC3II. LC3I is a precursor protein, which is distributed in the pulp. When autophagy occurs, LC3I is bound to phosphatidylethanolamine under the interaction of autophagy associated gene 7 (Atg7) and Atg12-Atg5-Atg16L, then hydrolyzes a small segment of the polypeptide to become LC3II, which is called autophagosome and binds to the autophagosome membrane. The molecular weight of LC3II is smaller than that of LC3I. Therefore, occurrence of LC3II indicates autophagy. Higher LC3II expression indicates higher level of autophagy. Therefore, the LC3II/I ratio in cells is able to determine the degree of autophagy.(26) In this study, LC3II/I protein ratios in the COPD group were significantly increased, indicating that autophagy occurred in the COPD group under the circumstance of similar LC3 gene distribution. This result is consistent with the study reported by Sukkar et al.(27) We also found that both gene and protein expression levels of P62 were significantly increased in the COPD group. P62 protein, also known as sequestosome 1, is an ubiquitin-binding protein encoded by SQSTM1, and acts as an autophagic substrate during autophagy,(28) playing an important role in the autophagic process.(29) The previous studies of a Ubiquitin Related Area (UBA) in this protein revealed that P62/SQSTM1 has been associated with protein degradation.(30) After the formation of autophagosome LC3II, P62 can guide LC3 protein to link with the autophagosomal membrane and form autolysosomes, followed by degradation of P62. Usually, the production and degradation of P62 maintain an equilibrium at normal levels of autophagy. Excessive increase of autophagy and interruption of the degradation of autophagic products cause P62 to pile up.(31) P62, therefore, is often used to detect the patency of autophagosomes and autophagy flow, and P62 and LC3 are simultaneously used to assess autophagy level in cells.(32) Recent studies showed that occurrence of various diseases is related to P62 accumulation in cells.(33–36) Assessing the neurodegenerative changes, it was found that autophagy is inhibited, resulting in P62 accumulation and increased formation of P62 corpuscles.(32) As a consequence, the intracellular signal transduction and activation of Keapl occurs, initiating the oxidative stress and tissue damage. P62 also activates the casepase8 apoptotic pathway, which initiates apoptosis.(37) Besides, several studies revealed that the expression of P62 is increased when the autophagy is elevated.(38–40) In addition, Shen et al. reported that P62 expression is negatively correlated with autophagy.(41)
In this study, the increased expression of LC3 in the COPD group supported autophagy elevation, and the pathways of downstream autophagy were smooth without obstruction. The increased P62 expression suggested that the excessive autophagy caused P62 accumulation., The increased autophagy in COPD patients in combination with the oxidative damage principle caused by P62 accumulation in the abovementioned diseases, leaded to elevated P62 accumulation. This may be contributed to the occurrence of alveolar oxidative damage.(11)
Next, we used flow cytometry to investigate CD8+ T cell subsets, and found that patients with stable COPD had significantly higher amounts of CD8+ T cells in peripheral blood than that in the SN group and NSN groups. The numbers of effector and memory T cells were also significantly increased. Meanwhile, the apoptotic rate of CD8+ T cells was reduced. Current studies have found that CD8+ T cells infiltrated in alveolar walls, the airway epithelium and the lung tissue are in an elevated state during remission from COPD.(11–13, 42, 43)
Then, we performed a Pearson correlation analysis of LC3II/l and P62 levels and the numbers of CD8+T cells, including CD8+ effector and memory T cells, in stable COPD patients. There was a moderate positive correlation between increased autophagy level and elevated amounts of CD8+ T cells. CD8+ T cell autophagy was increased in patients with stable COPD, promoting the survival of CD8+ effector T cells and the formation of memory T cells, therefore, the overall cell number increased.(21, 22) These result demonstrate that autophagy may be one of the main factors that increased the amounts of CD8+ T cells in peripheral blood in patients with stable COPD.
Of not, it was also found that CD8+ T cell autophagy in patients with stable COPD was increased, yet the apoptosis was reduced. Autophagy and apoptosis are both cell death processes, which are different from necrosis. However, the causes and mechanisms of autophagy and apoptosis are different. Autophagy is mainly used to eliminate waste cell organelles, and forms autophagy lysosomes with no typical characteristics of apoptosis such as nuclear condensation, nuclear rupture, cell shrinkage, and formation of apoptotic bodies. It is therefore called autophagic cell death, representing a new type of programmed cell death. To distinguish it from apoptosis, autophagy is termed Type I cell death, while the apoptosis and necrosis are regarded as Types II and III cell death, respectively. Autophagy is associated with both cell survival and death. In some cases, it is involved in cell death, while the autophagy promotes cell survival in other cases.(44) The relationship between autophagy and apoptosis is relatively complex, and the specific mechanism has not been fully understood. Under the normal conditions, the autophagy rarely occurs in cells unless there are predisposing factors such as starvation, the lack of growth factors, ischemia and hypoxia, microbial infections, etc. In some cases, autophagy is an adaptive mechanism under stress conditions; cells remove impaired mitochondria by autophagy, increase the ability of anti-hypoxia, and prevent the necrosis and apoptosis. Hence, under reasonable stress conditions, autophagy exerts a protective effect on cells. However, the excessive autophagy may damage cells and cause cell death. Previous studies reported that the increased autophagy promoted the the formation of CD8+ effector and memory T cells.(6, 7) In this study, autophagy level, the total number of CD8+ T cells, as well as the amounts of effector and memory T cell, were increased in patients with COPD, while the apoptotic rate was decreased. We considered that the autophagy of CD8+ T cells was increased in patients with COPD, repairing organelle damage and preventing cell necrosis or apoptosis. As a result, the overall rate of cell survival increased, and the apoptotic rate decreased. The Autophagy promoted the survival of CD8+ effector T cells and the generation of memory T cells, and the overall number of cells increased. Therefore, there is no contradiction between the autophagy and apoptosis. These results suggested that the number of CD8+ T cells was positively correlated with autophagy level in these cells. However, the irrespective of apoptotic level, indicated that the amounts of long-term CD8+ T cells increased in stable COPD patients may because of the elevated autophagy levels rather than the decreased apoptotic rate.
Furthermore, we found that the amounts of CD8+ T cells and the expression levels of the autophagy associated proteins LC3II/l and P62 in SN group were higher than those of NSN group. Currently, several studies reported that smoking is in relation to the amounts of CD8+ T cells. Compared with non-smokers, smokers showed increased amounts of CD8+ T cells infiltrated into the bronchial epithelium and the lung tissue.(5, 7) Previous studies also found that smoking are able to promote autophagy(16, 17), resulting in emphysema.(15–19) Yang et al. found that in nicotine-controlled human periodontal ligament cells, autophagic level is significantly increased.(45) All of these study demonstrated that smoking promotes autophagy. It is likely that smoking promotes the survival of effector T cells and the formation of memory T cells through increase of autophagy, leading to a long-term increase in amounts the CD8+ T cells and maintaining such increase even after smoking quitting.(3, 4) Next, we plan to treat cells with tobacco extracts, and observe the dynamic changes of autophagy levels and amounts of T-cells, to further explore the correlation between smoking and autophagy.
At the beginning, this study was designed as a controlled study of COPD and non-COPD patients. The COPD group was not further divided into acute and remission stage groups, mainly because that acute infection can greatly induce autophagy. However, after reviewing the study, a limitation of this study was that if the COPD group was divided into acute and remission stage groups, we could detect changes of autophagy levels and amounts of CD+8 and CD+4 cells between both phases, which might provide additional insights. The other one limitation of this study is that the indicators used to detect autophagy were relatively simple. Only the ubiquitous autophagy associated protein LC3 and the autophagy degradation protein P62 were utilized, and a number of proteins that reflect the autophagy level were not included due to limited research funds. Future studies will address the these issues.
{kind=link}