Setting
The Taiwan Ministry of Health and Welfare (MoHW) adopted the categorization, designation, and regionalization international guidelines to establish a national emergency care system, including prehospital emergency medical services (EMS), emergency medical responder-responsive hospital designation, regionalization, and categorization of hospital emergency capability. Taiwan’s ED regionalization and categorization policies were implemented in 2007 and 2009, respectively, with the primary goals of establishing infrastructure and decreasing regional disparity.
Study Design and Timelines
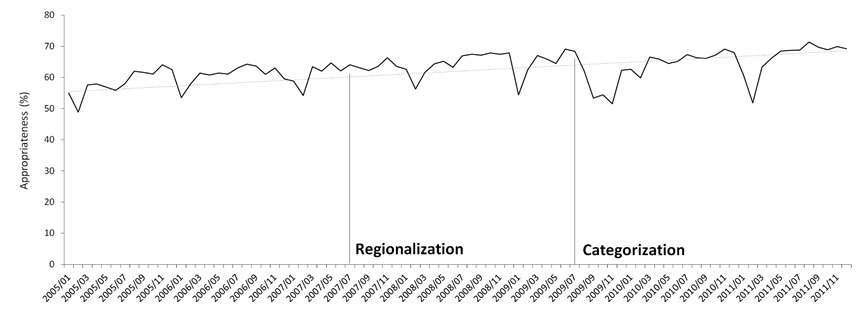
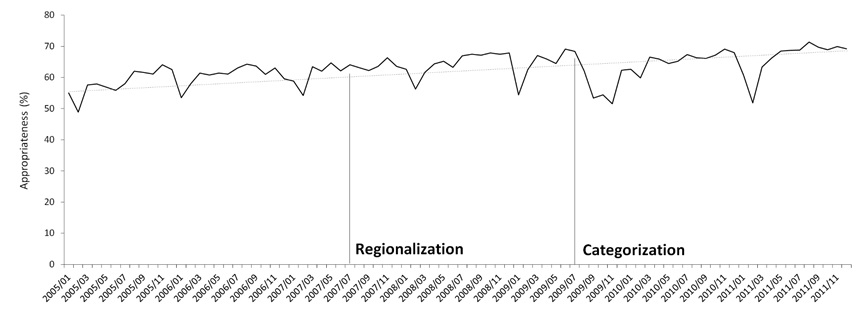
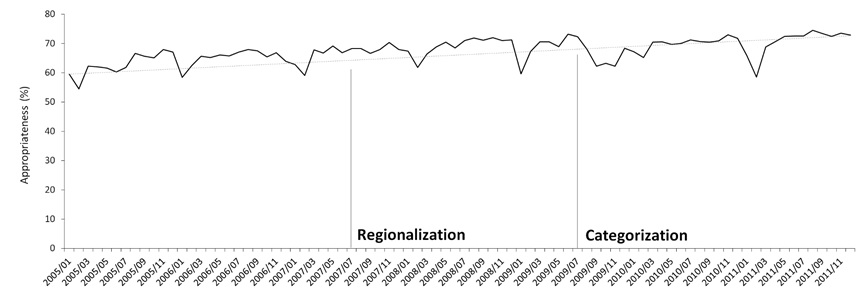
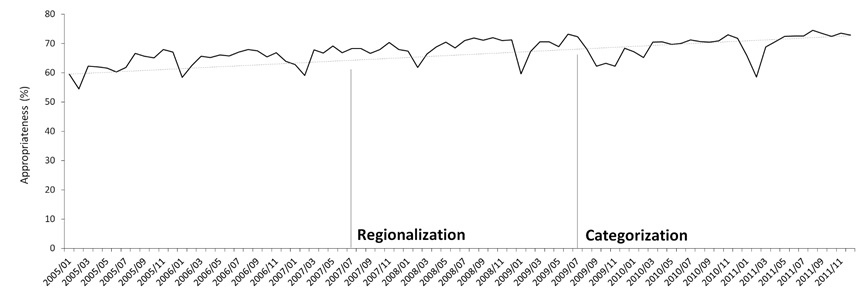
This seven-year retrospective observational study on the effect of hospital emergency care policies on patient-appropriate ED use included all ED visits between January 1, 2005 and December 31, 2011. Each visit date was associated with one event to avoid replicating events (Figure 1). We divided the study period in three: the pre-policy period (October 2005–July 2007), regionalization policy intervention period (August 2007–July 2009), and categorization policy intervention period (August 2009–July 2011).
Regionalization Policy
The regionalization policy focuses on prehospital EMS networking and rescuer-responsive hospital ED designations. Its primary objective was to increase the accessibility of emergency care. To achieve this objective, health authorities first identified responsible hospitals in 61 subregions; subsequently, every subregion had at least one hospital that was designated to respond to acute events.
In July 2007, Taiwan launched the Emergency Medical Services Act Amendment. The revised Emergency Medical Services Act represented a landmark for reorganizing the network of emergency care systems in Taiwan; this act implemented three significant changes: (1) introducing hospital-based ED categorization focused on ED medical capability to provide resuscitation, (2) establishing a medical director system to connect hospital ED physicians with prehospital EMS, and (3) forming six regional emergency operations centers (REOCs). Prehospital regionalization efforts included onsite auditing by the MoHW and the categorization of hospital-based ED using a three-tiered approach to emergency care (severe, moderate, and general). Moderate- and severe-tiered EDs undergo onsite audits by the MoHW, while general-tiered hospitals are overseen by the local health authority.
The hierarchical system of emergency rescuer-responsive hospitals and designated hospital ED must provide transport within 30 minutes for time-sensitive events such as stroke, acute myocardial infarction, major trauma, high-risk pregnancies, and newborns. Six REOCs may dispatch EMS ambulances and rescue personnel from local hospitals to emergency patients and mass casualties. The REOC coordinates with the EMS to provide onsite prehospital triage and care, and dispatches patients to the nearest designated appropriate hospital ED.
Categorization Policy
In 2009, the Taiwan MoHW promulgated the “Standards for the categorization of hospital emergency capability.” According to these standards, the MoHW categorized hospitals into three tiers (severe, moderate, and general) based on their emergency care capability and capacity (including hospital ED, critical time-sensitive-event care teams, and intensive care unit). The primary focus of this policy was the establishment of centers for trauma, cardiac catheterization, stroke, perinatal emergency care conditions, high-risk pregnancies, and pediatric intensive care.
The Joint Commission of Taiwan accredits hospitals every four years, and severe-tiered hospitals are considered the last line for hospital referrals. At the end of 2009, 191 rescuer-responsive hospitals were accredited, including 26 severe-, 76 moderate-, and 89 general-tiered hospitals. This policy ensures the use of timely, continuous, effective, and collaborative multidisciplinary methods with two principal objectives: (1) to provide quality hospital emergency care, and (2) to provide a hospital emergency care capability classification with information regarding whether patients chose the appropriate treatment setting (right care in the right place). This information provides patients with appropriate quality information to increase the appropriate ED use. Therefore, the prehospital EMS, hospital ED, hospital emergency care teams, and intensive care unit critical care capability and capacity were well established and categorized in Taiwan [36].
Estimated Appropriate ED Use
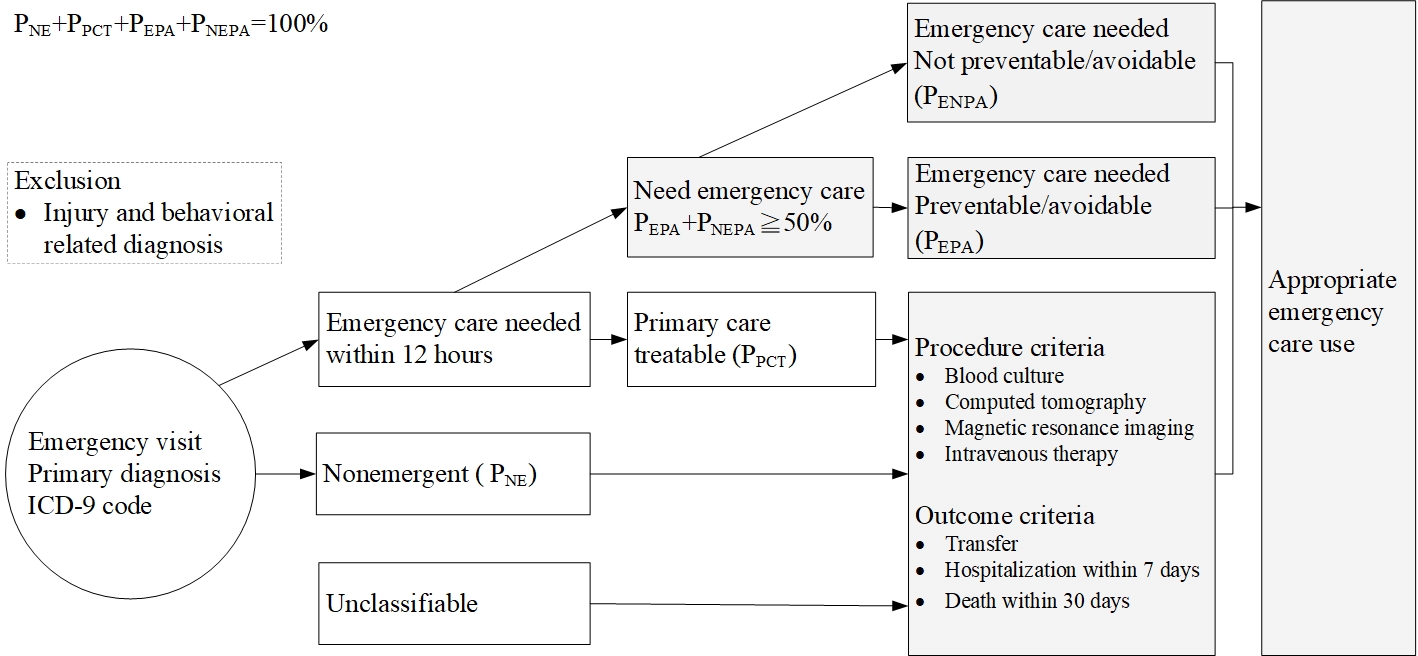
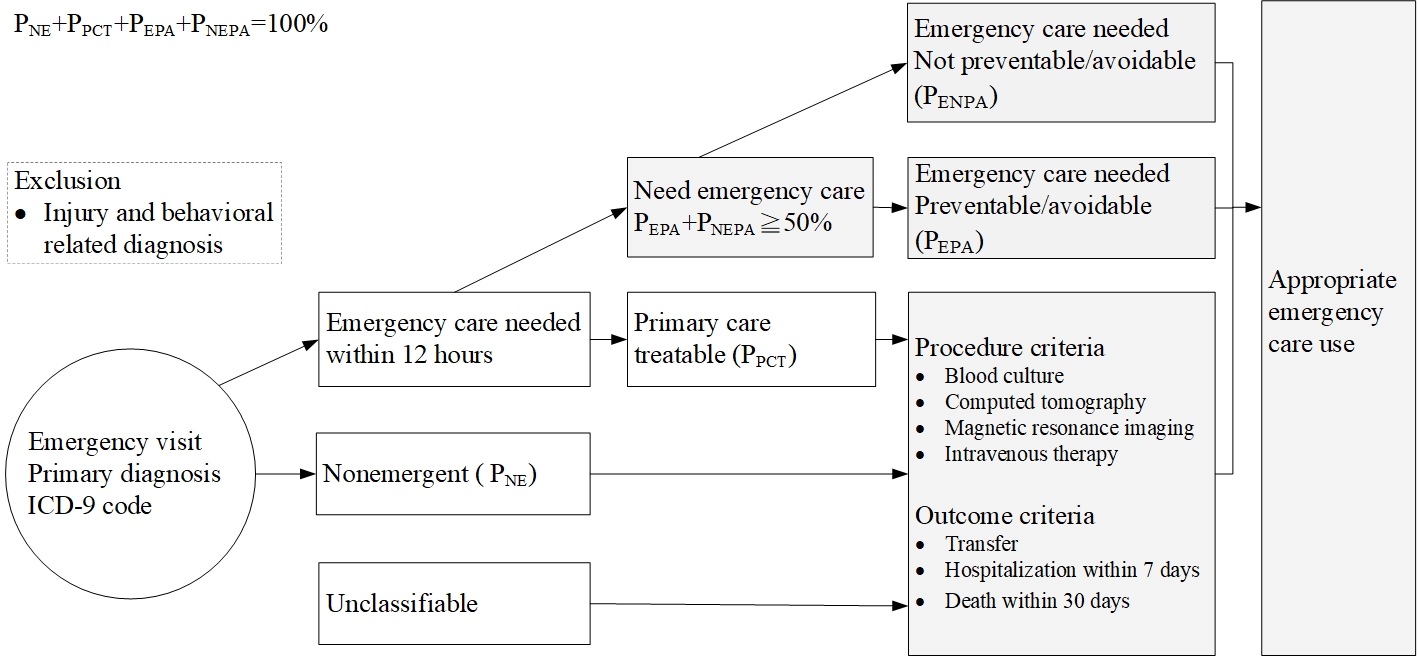
We used a revised version of the Modified Billings/New York University-ED algorithm (NYU-ED algorithm) for emergency care evaluation according to processes and outcome indicators—referred to as the Yang-Ming modified NYU-ED algorithm—to define the appropriateness of ED use (Additional Figure 1) [37]. This algorithm classifies ED visits as emergent vs. nonemergent, and optimal care site as ED vs. primary care. It further divides an ED visit into six categories: (1) “nonemergent” (NE), (2) “emergent, primary care treatable” (EPC), (3) “emergent care needed, preventable/avoidable” (EPA), (4) “emergent care needed, not preventable/avoidable” (ENPA), (5) unclassifiable, and (6) “injury and behavioral health-related diagnosis” [38].
The Modified Billings/NYU-ED algorithm classifies ED use as appropriate when EPA and ENPA summative primary diagnosis probabilities are equal to or greater than 0.50, whereas NE and PCT are classified as inappropriate ED use [39-41].
We reclassified inappropriate and unclassifiable ED visits using explicit procedures (if a patient received any procedure that is not often available in primary care settings, such as computed tomography or magnetic resonance imaging scans), and outcome-based criteria (if a patient is transferred, hospitalized, or dies) to reflect the complexity of a patient’s condition and appropriateness of emergency care usage. Injury and behavioral health ICD-9 codes were excluded as the original Billings/NYU-ED algorithm[38].
Data Access and Covariates
The analytic data were derived from the Taiwan Longitudinal Health Insurance Database 2005 (LHID2005), which is maintained with routinely collected administrative data from the National Health Insurance [42, 43]. The LHID2005 comprises one million randomly sampled participants who were alive in 2005; the database includes all medical records for these individuals from 1995 onward. It also includes hospital and medical professional staff characteristics, subject enrollment, and medical information. This database reflects healthcare facilities’ accessibility and medical care utilization [44, 45]. The collected medical utilization information includes diagnosis procedure, treatment medication, medical cost, date of visit, and deposition [46]. The accuracy of the diagnoses recorded by the LHID2005 for time-sensitive diseases, such as acute ischemic stroke [47, 48], acute myocardial infarction [48], asthma [49] and pneumonia [50], has been validated. Encrypted unique personal identification numbers link all the data, allowing a longitudinal follow-up.
We identified ED visits using the ED visit case type and revenue codes. We used these data to count ED visits. We obtained visit-level data for all ED visits to all hospitals in Taiwan from 2005 to 2011. The covariates included predisposing factors such as sex, age, and occupation; enabling factors such as the beneficiary’s insured salary, urbanization of living area, and emergency care resources classification; and need-driven factors such as comorbidity status. Comorbidity status was defined using the Charlson Comorbidity Index (CCI) score [51].
Statistical Analyses
We compared the two policy periods’ baseline covariates characteristics using χ² tests and t-tests accounting for the LHID2005 administrative data. Because ED use and its covariates are time-dependent and longitudinal, we performed a time series analysis to estimate multilevel changes in appropriate ED use rates after regionalization and categorization policy interventions. Before examining the policy’s effect on appropriate ED visit rates, the Dickey-Fuller test was used to determine the baseline appropriate use rate. The difference in monthly mean probabilities after hospital ED regionalization and categorization was determined using a segmented autoregressive integrated moving average (ARIMA) model with an indicator variable for the regionalization and categorization periods. This model can examine the policy intervention effect while accounting for autocorrelation and time effects. We also evaluated the odds of having an appropriate ED visit during the regionalization and categorization policy stage compared with previous policy stage. All analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC) and Stata MP 14.0 (StataCorp LLC, College Station, TX) software. Statistical significance was determined using a two-tailed significance level of 0.05.
Sensitivity and Bias Analyses
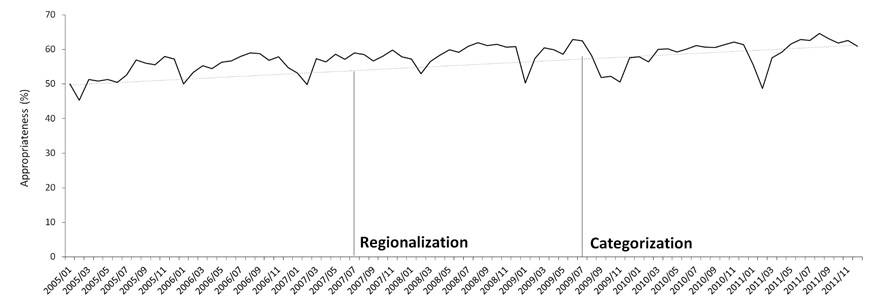
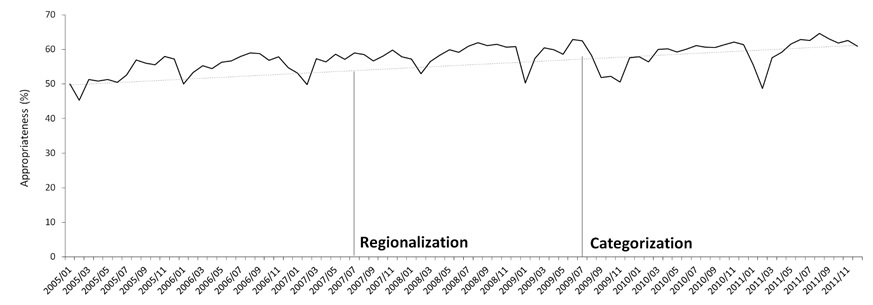
According to a systematic review on ED crowding, the common causes of input factors are nonurgent visits, frequent flyers, and influenza season [52]. During our study period, no specific ED-related policy was promulgated nor was the ED co-payment scheme changed. We evaluated the effects of frequent ED users (≥ 4 visits per year) [53] (Additional Figure 2) and the 2009 influenza season (Additional Figure 3) [54]. Excluding the effects related to these factors, the trend in appropriate ED visit classification showed no substantial changes. A sensitivity analysis was conducted increasing the threshold of EPA and ENPA summation probabilities to ≥ 0.75 (Additional Figure 4). Similar trends in ED visit classification further demonstrated the lack of significant changes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}