The objective of this study was to assess the impact of 18 years of IVM-based preventive chemotherapy (PC) on the prevalence and intensity of L. loa infection in the Yabassi Health District in the Littoral Region, Cameroon.
The Yabassi Health District belongs to the Littoral CDTI project, and treatments with ivermectin have been initiated in that area since the years 2000s to fight onchocerciasis. Indeed, IVM is a macrocyclic lactone acting by killing almost 70–80% L. loa microfilariae within the first three days after a single dose of the drug, a total clearance being observed within 4–5 days in some individuals [29–30]. In addition to its principal effect (microfilaricidal), IVM also prevents for about three months the release of new microfilariae by adult female worms, so-called embryostatic effect. However, ivermectin is not adulticidal, though some macrofilaricidal efficacy has been described in the treatment of O. volvulus - a filarial parasite closely related to L. loa - after repeated doses of IVM [31]. Since L. loa adult worms are lifelong (lifespan estimated up to 15–17 years) [32], repeated treatments with IVM are likely needed to interrupt the transmission of this filarial disease, the number of rounds of treatment remaining unknown. The long-term (18 years) implementation of CDTI in the Yabassi Health District likely explain the marked decrease observed in both prevalence and intensity of L. loa infection as was already observed elsewhere in Cameroon [23].
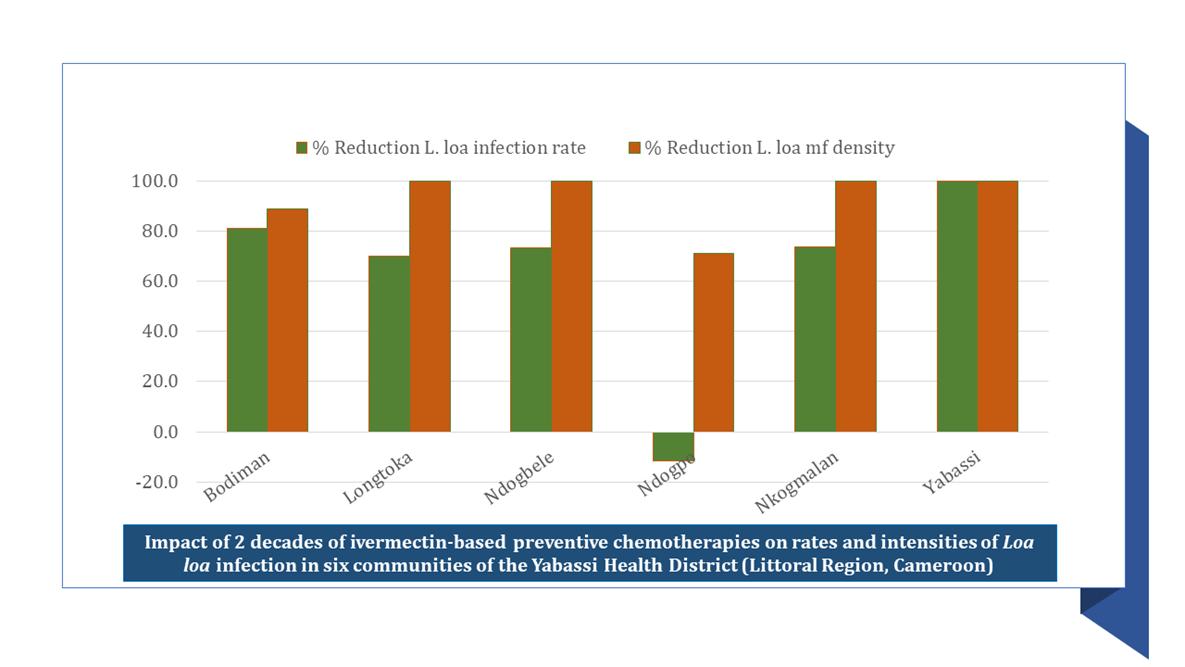
The percentage differences were more important for infection rates (-70.2%) compared to intensity of infection (-99.8%), likely indicative of the fact that adult worms are life-long and producing microfilariae for their whole life. As such, repeated doses of IVM will reduce the productivity of adult worms and therefore the microfilarial densities, but prevalence will remain almost unchanged, especially during the first years/rounds of treatments. This can also support why percentage differences are also low among the youngest individuals. The impact of IVM on parasitological indicators of Loa loa infection (prevalence and microfilarial density) was also found to be highly variable among communities (Tables 1 and 2), likely related to adherence to treatments. Indeed, communities where the highest percentage reductions in Loa loa prevalence and microfilarial densities were found exhibited higher proportion of fully compliers and lower proportions of permanent non compliers.
None of the patients interviewed remembered having experienced Calabar swelling and migration of adult worm under the bulbar conjunctiva, which are the most common clinical signs of loiasis used for rapid mapping of loiasis [26]. Indeed, it has been previously demonstrated that apart its direct effect on parasites, IVM exhibits a beneficial effect on the clinical manifestations of loiasis, by for example preventing the reappearance of Calabar swelling for several months [33]. This likely suggests that these enrollees might have experienced these clinical signs very long time ago and might be victims of memory bias. Only few participants declared suffering from pruritus; although this can be likely due to the low level of L. loa microfilarial densities observed in the framework of this study, it is important to mention that this clinical manifestation is shared with other filarial diseases, and Yabassi Health District is known to be endemic to onchocerciasis [34].
Despite the significantly high decreasing trends observed both in rates and intensities of infections, the transmission of the disease was still ongoing even though the endemicity level was quite low. This slight persistence of the disease can be explained by the presence in the communities of systematic non compliers, who can disseminate the disease and contribute to the persistence of the infection if infected, especially in a context where the chrysops vectors of L. loa are known to be highly competent [24; 35]. Importantly, some enrollees exhibited very high L. loa microfilarial densities and are therefore at risk of developing severe adverse events (SAEs) if treated with IVM. This suggests that despite multiple rounds of IVM, the risk of developing SAEs is still present, especially among those individuals receiving IVM for their first time or who have interrupted treatment for a while, whatever the reason. Onchocerciasis and Lymphatic Filariasis control or elimination programs should consider testing for loiasis before administering IVM to all those involving in CDTI for their first time, and this can be made possible by the recently developed “Test and Not Treat” procedure [36–37].
{kind=link}