Although only few chondroblastoma of the rib has been reported in the English literature, there are no definitive or standard treatment guidelines. Only rare cases reported that described the diagnosis, radiographic and histological findings, treatment, and follow-up.
Local pain is the most common symptom of chondroblastoma. Other signs and symptoms include in swelling, effusion or pathological fractures on rib, physical examination may show swelling and local tenderness [3, 5]. The case did not describe any pain or discomfort associated with the tumor, and we believe this was because the tumor was small and there was no invasion of adjacent tissues or intercostal nerve involvement.
CT and Magnetic resonance imaging (MRI) are helpful in making a diagnosis [8]. CT may reveal cortical thinning, cortical expansion with erosion, a periosteal reaction, and calcifications in center of the tumor; unusual radiographic changes may also be seen [1]. It can provide the tumor size and identify extension of the lesion into cortical bone, and it is helpful for planning surgery. MRI can identify a soft tissue mass and medullary invasion, and the tumor presents as low signals on T1-weighted images, and with less inhomogeneity and high signals on T2-weighted images. MRI is useful for determining the extent of the tumor, and identifying pathological fractures within the lesions. On contrast-enhanced MRI, the tumors exhibit lobular, marginal, and septal enhancement [9].
Chondroblastoma is relatively benign tumors, and microscopic examination reveals typical polygonal-shaped chondroblasts and osteoclast-like giant cells. HE shows chondroblasts that are large and closely packed with a central, characteristically translucent cytoplasm and grooved nucleus. In general, chondroblasts and osteoclast-like giant-type cells will be observed [3]. Scattered throughout are small, nucleated giant cells and islands of more mature cartilage. Mitotic features can be present, but are sparse among the generally well-defined nuclei. Calcifications are typically present, and have an intercellular distribution with a "chicken wire" or "picket fence" appearance [2].The chicken-wire pattern of calcification is helpful in making a firm diagnosis. However, it is not present in the majority of lesions making it a secondary diagnostic criterion. IHC staining for S100 or K36M is positive in chondroblastoma, and is a useful ancillary method for making a diagnosis of chondroblastoma [9, 10].
Chondroblastoma belongs to a benign tumor, locally aggressive tumor surgery plays a role in all treatments. Some studies also suggested that chondroblastoma of flat bones are more aggressive than those in long bones [11]. Recurrence after surgery is reported to occur in 10–36% of cases [1, 12], and recurrence rates approaching 20% have been reported even with complete resection [5]. In our case we did not perform traditional open thoracic surgery instead of VATS resecting the tumor and broken rib with a wire saw. Intraoperative frozen section pathological examination confirmed that the margins of the resected specimen were negative. Compared with the traditional surgery, VATS is minimally invasive and only requires two small incisions, has little or even no impact on lung function, and is associated with a reduced requirement of analgesics, shorter chest drainage tube time, and shorter hospital stay postoperative. In addition, postoperative chest wall numbness is less than that with traditional open thoracic surgery. Earlier reports have advocated curettage for the removal of the tumor [13], but increased recurrence rates have been reported when only curettage is performed for the aggressive tumors [11]. Complete resection is necessary for aggressive tumors (as in our patient).
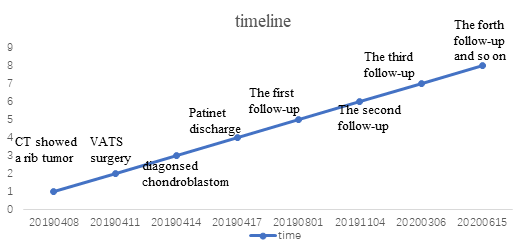
To reduce the risk of recurrence and metastasis, close and regular follow-up is necessary postoperative. Imaging studies are useful for early diagnosis of tumor recurrence. Follow-up can include physical examination and chest CT every 3 months, and bronchoscopy, abdominal ultrasound, brain MRI, and a bone scan every 6 months for the first 3 years is necessary, then every year to 5 years postoperatively [13]. Close and extensive follow-up may improve the outcomes of patients through detection of asymptomatic recurrences and metastasis.
Radiotherapy is a treatment option for patients who are poor surgical candidates, and for patients with recurrent or unresectable disease, and prevent the recurrence, but which is not a standard method treatment[10]. Radiotherapy is not recommended after complete resection, due to the possibility of radiation-induced chondrosarcoma [6]. At present, there is no role for chemotherapy in the management of chondroblastoma [8].
Metastasis most frequently involves the lungs, tends to occur at the time of primary tumor recurrence, and may be present at the time the bone lesion is identified. Lung metastases are clinically non-progressive, and can be treated by limited surgical resection or simple observation.
The primary limitation of this report is the short follow-up time; longer follow-up is necessary to evaluate the efficacy of treatment.