This retrospective monocentric study was approved by the Ethics Committee of Foch Hospital affiliated to Paris Ouest University, and the requirement for informed consent was waived.
Patients
Three hundred and nineteen consecutive patients examined at the Emergency department between March 20 and April 8 2020 underwent a CT scan of the chest because of intermediate clinical probability of COVID–19 pneumonia. Intermediate clinical probability was defined by typical or atypical clinical presentation (no typical finding at auscultation despite respiratory symptoms), but a normal or equivocal chest X ray. In the same period of time, 225 patients were hospitalized without a CT scan because of typical clinical and radiographic findings of COVID–19 pneumonia, and 645 patients were not on the basis of clinical evaluation and chest X ray.
CT scans
A CT room was fully dedicated for patients suspected of having COVID–19 accessible from the Emergency department through a well delineate route. CT gantry and every potentially contaminated surface was disinfected after examination. Unenhanced low dose volumetric acquisition was performed over the entire chest at full inspiration in all patients. Contrast injection was used in 53 patients because of suspicion of pulmonary embolism associated with COVID–19. Contiguous 0.6 mm axial images were reconstructed with high resolution and soft tissue kernels.
Radiologist readings
Two independent chest radiologists (ALB and PAG) with 15 and 30 years of experience reviewed CT examinations being blinded for RT-PCR results and any clinical information except patient sex and age. They read the images using lung window and mediastinal settings on the PACS system (GE).
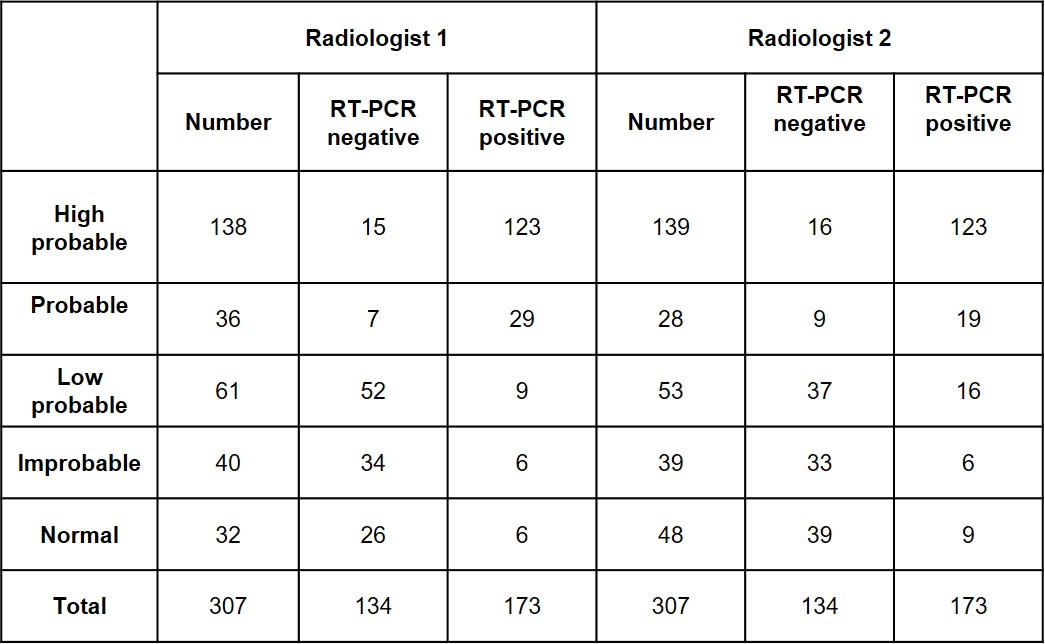
The radiologists were asked to classify the CT scans as: high probable, probable, low probable or improbable diagnosis of COVID–19 pneumonia, or normal. They established their diagnosis as high probable and probable on the basis of the recent publications from China illustrating typical and atypical patterns observed in patients with COVID–19 pneumonia [4–9, 15–19]. Low probable diagnosis was defined by the presence of parenchymal abnormalities, which did not fit with the diagnosis of COVID–19 pneumonia nor with any other alternative diagnosis. Improbable diagnosis included typical patterns of infective or non infective lung diseases that might explain the patient’s symptoms (ie. lobar pneumonia , bronchopneumonia, infectious bronchiolitis, infected bronchiectasis, interstitial lung disease, heart failure or malignant tumor). Pulmonary emboli was considered an alternative diagnosis if not associated with any parenchymal abnormalities suggestive or COVID. If associated with evidence of COVID, the CT was considered high probable or probable depending on the associated pattern. A normal chest CT scan was the last possible option, keeping in mind it does not exclude early COVID–19 pneumonia.
RT-PCR
Viral ARN was detected in nasal swabs. The real-time reverse transcription-polymerase chain in reaction (RT-PCR) of viral nucleic acid was used as the reference standard for the diagnosis of COVID–19 infection. In 296 patients RT-PCR assay was performed in our hospital by nasal swab with a technique based on a reagent containing three viral targets (PCR Seegene Allplex. Eurobio). In ten patients RT-PCR was performed in a different laboratory before patients arrived on site. In 13 patients RT-PCR was not available because of an alternative diagnosis suggested by CT scan or because the patient was transferred to another hospital.
Statistical analysis
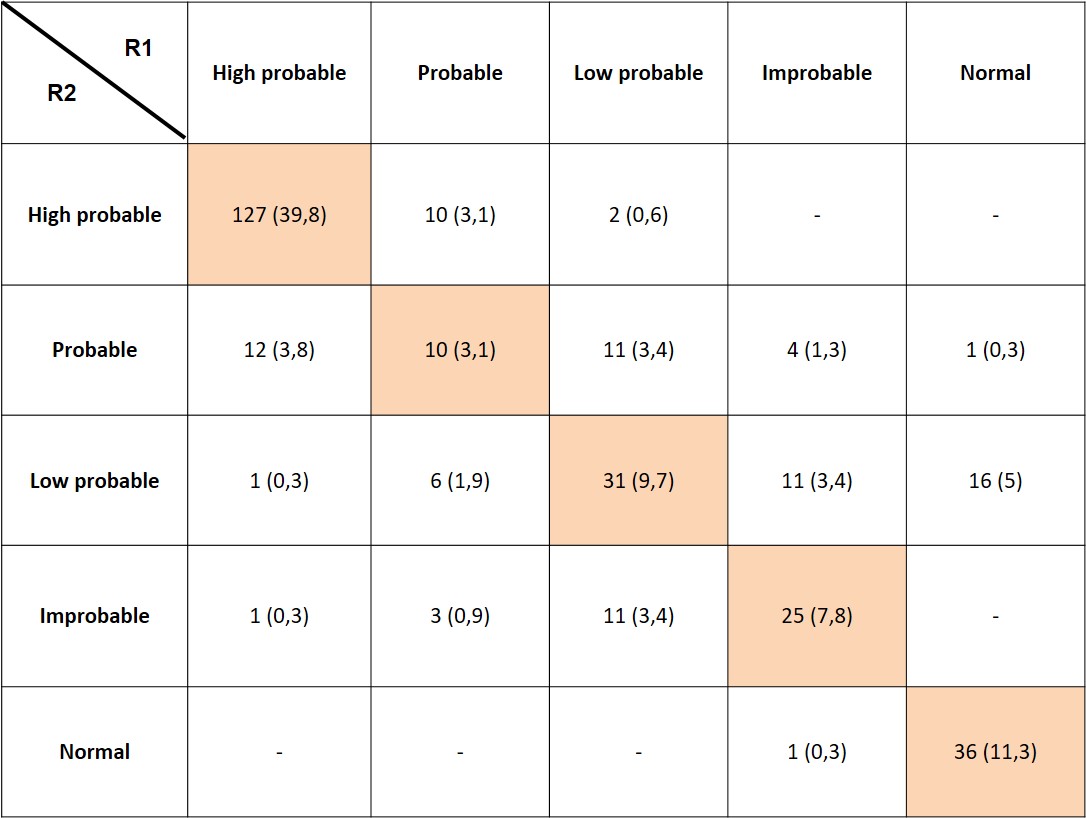
Concordances and discordances between the two radiologists for the diagnosis of COVID–19 pneumonia were assessed using kappa statistics. The values of kappa can range from +1 (almost perfect agreement) to –1, where 0 represents the amount of agreement than can be expected from random chance [20].
The result of RT-PCR was used as the ground truth for measuring CT diagnostic accuracy. Because of the limited sensitivity of RT-PCR reported in the literature, clinical management and outcomes of patients with a negative RT-PCR and a CT scan classified by both radiologists as «high probable or probable» for COVID–19 pneumonia were reviewed. On the basis of this analysis, patients were considered as definite COVID negative or reclassified COVID positive.
Receiver operating characteristics (ROC) was plotted and the area under the curve (AUC) was calculated with 95% confidence intervals for each radiologist.
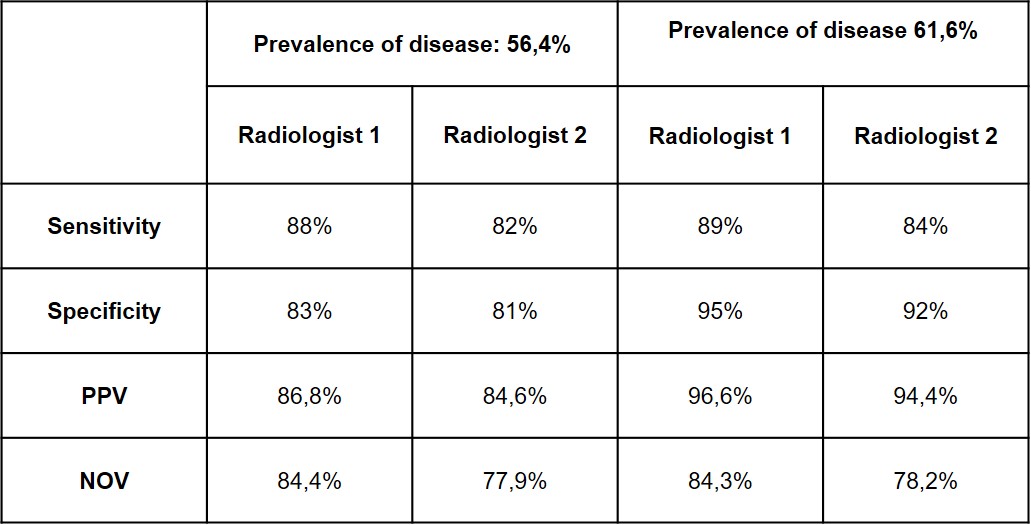
Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for both radiologists
PPV and NPV were calculated with the following formula [21]:
PPV = Sensitivity x Prevalence / Sensitivity x Prevalence + (1-Specificity) x (1- Prevalence)
NPV = Specificity x (1-Prevalence) / Specificity x (1-Prevalence) + (1-Sensitivity) x Prevalence
{kind=link}
{kind=link}
{kind=link}