Traditional treatments for EC, such as surgery, radiation therapy, and chemotherapy, have a significant impact on patients’ quality of life and are associated with low effectiveness rates,29 warranting, new effective therapeutic approaches. Immune checkpoint inhibition and CAR T-cell therapy have improved cancer immunotherapy,30 providing patients with hope for a possible cure. Owing to the heterogeneity of each patient’s tumor-suppressing microenvironment, immunotherapy is only effective against a subset of tumors, and only a small percentage of patients with cancer successfully respond to immunotherapy.31 However, the use of biomarkers to predict immunotherapy responses accurately can enable personalization of immunotherapy for each patient.32 To this end, LPXN may be a dependent indicator of immunotherapy efficacy and a potent prognostic biomarker of ESCC.
We evaluated LPXN expression in EC/ESCC using data from GEPIA and UALCAN and found that ESCC dramatically increased LPXN expression. In vitro molecular studies were performed to confirm the results because of uncertainty regarding the accuracy of the bioinformatics analyses. q-PCR and IHC results were supported by the gene expression profiles of LPXN in EC/ESCC from the GEPIA and UALCAN databases. In patients with EC/ESCC, high levels of LPXN gene expression were linked to poor prognosis, indicating that LPXN may be a risk factor for this condition. The relationship between OS and pathological staging supports this conclusion. Comprehensive cell tests were performed to confirm this finding, wherein LPXN knockdown resulted in fewer active ESCC cells, increased apoptosis, and impaired migration and invasion capacities compared with cells transfected with an empty vector. Overall, our results show that LPXN, which functions as both an oncogene and a potential prognostic biomarker, has a critical role in ESCC initiation, development, and progression. However, information on whether LPXN is connected to ESCC is limited. In determining the prognostic and indicative value of LPXN in ESCC, our study is the first to combine bioinformatics analysis, RNA sequencing, cell experiments, and IHC. The findings of this study establish a connection between LPXN gene expression levels, prognostic indicators, and the effectiveness of immunotherapy.
LPXN has been a potential biomarker for various cancers.12,14,33–36. Some of these studies have focused on PCa. LPXN functions in PCa invasion and development by interacting with the androgen receptor (AR). Khan et al.37 studied the AR-LPXN coupling pathway in PCa. Using artificial intelligence to analyze gene expression data, Carreras et al.38 suggested that LPXN could prevent the development of diffuse large B-cell lymphoma. Conversely, inhibiting LPXN expression blocked MMP-2 and MMP-9 release, activated the cJun NH2-terminal kinase pathway (JNK) and mitogen-activated protein kinase signaling pathway (p38 MAPK), and halted the malignant growth and transmembrane invasion of human acute monocytic leukemia SHI-1 cells. LPXN overexpression may be involved in the proliferation, adhesion, and invasion of human acute monocytic leukemia THP-1 cells.39 New insights into potential therapeutic targets for bladder cancer were provided by Hou et al.,40 who discovered that LPXN may enhance bladder cancer growth by upregulating the expression of S100P via phosphatidylinositol 3kinase/protein kinase B signaling. The results for cervical, ovarian, uterine, endometrial, bone, kidney, and lung cancers were all comparable.41–45 These results suggest that LPXN functions in oncogenesis.
Several clinical trials, including CheckMate-577,46 CheckMate-648,47 ESOPEC,48 TOPGEAR49, Keynote-181,50 Keynote-590,51 RATIONALE-306,52 ASTRUM-007,53 and JUPITER-06,54 have demonstrated that efficient targeted immunotherapies may significantly improve EC patient survival outcomes. To ascertain the likely mechanism by which LPXN affects survival outcomes and build a framework for future molecular investigations, GO and KEGG enrichment analyses were performed.
Cancer cells are now understood to be embedded in connected stromal cells, which involve vascular cells, fibroblasts, and inflammatory immune cells forming the tumor microenvironment.55 This definition is a considerable shift from the “cancer cell-centered” perspective that previously dominated the field. A link between LPXN, stromal score, and immunological score was identified using the ESTIMATE method. LPXN is probably secreted by stromal cells or participates in stromal processes because of its association with the stromal score. The strong connection between LPXN and the immunological score suggests that tumor tissues with high LPXN expression may be invaded by the immune system.
Cancer stem cell-like cells56 originate from progenitor cells, non-stem cell dedifferentiation, and long-lived stem cells. They are responsible for treatment-induced drug resistance57 owing to their propensity to self-renew and infiltrate, thereby promoting tumor development. DNAss exhibited a strong correlation between LPXN expression and tumor stemness, suggesting that LPXN has a role in tumorigenesis.
Increased PD-1 and PD-L1 expression is useful in treating ESCC57 by reducing the antitumor immune response of T cells. Here, the expression of LPXN was positively correlated with that of PD-1 and PD-L1. Moreover, western blotting determined a positive correlation between LPXN and PD-L1 protein expression in ESCC cell lines.
To directly validate the link between LPXN and the success of immunotherapy in ESCC, we collected tumor samples from 22 patients who underwent immunotherapy at the Chongqing University Cancer Hospital. Based on various treatment responses, q-PCR and IHC staining revealed that LPXN was expressed in tumor samples from the treatment response group compared with those from the poor response group. Thus, LPXN expression can predict the levels of immunological checkpoint expression and influence therapeutic choices.
Multiple types of immune cells, such as macrophages, CD8+ T cells, and Th17 cells, are linked to cancer outcomes.58–60 Our analysis of data from the TIMER database demonstrated a connection between LPXN expression and B cell, CD4 + T cell, dendritic cell, macrophage, and neutrophil counts, suggesting the importance of LPXN in the tumor immune microenvironment. Many cancer types have experienced a dramatic shift in the clinical therapy landscape as the use of ICIs has become increasingly important in poor prognosis pathways.61,62 Therefore, we examined the relationship between LPXN and ICI gene expression and discovered that LPXN was associated with several ICI genes.
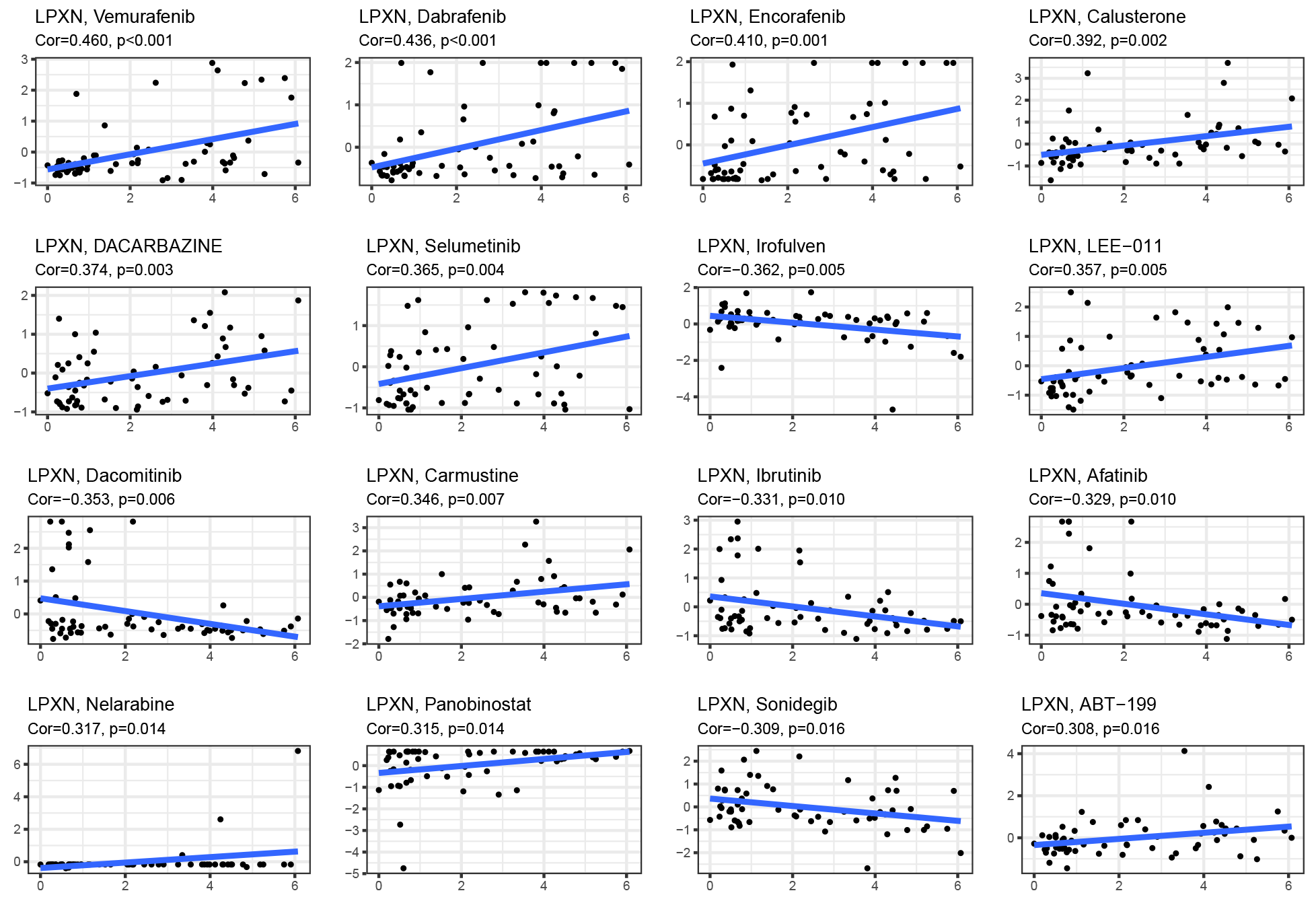
Based on the information on NCI-60 cell lines, elevated LPXN expression was associated with resistance to therapy with many chemotherapeutic agents with FDA approval. LPXN was linked to increased drug sensitivity to some medications, including vemurafenib, dabrafenib, encorafenib, calusterone, dacarbazine, selumetinib, LEE-011, carmustine, panobinostat, and ABT-199.
Among 13 members of the multidrug resistance protein (MRP) family, MRP1–MRP9 are the primary transporters contributing to multidrug resistance by obstructing chemotherapy uptake by cancer cells.56 Because of its relationship with MRP1, LPXN may serve as a therapeutic target for drug resistance and enhance drug sensitivity.
Our investigation remains subject to certain limitations. As a preliminary exploration of the correlation between LPXN and ESCC, this study suffers from a scarcity of related reference publications. Moreover, China presents a high prevalence of ESCC, principally ESCC, while Western countries observe a higher incidence of esophagogastric junction adenocarcinoma. Consequently, current leading databases provide few ESCC cases, and some instances lack comprehensive clinical data, impeding our ability to gather adequate cases for data scrutiny and reciprocal verification. For instance, when employing the GEPIA database to validate LPXN's differential expression in ESCC, we included several esophageal adenocarcinoma cases. Additionally, a dearth of clinical information precluded disease-free survival analysis from our survival examination. To address these shortcomings, we executed numerous experimental authentications of LPXN's biological role in ESCC using clinical specimens. Of note is the absence of any relevant mechanisms pertaining to LPXN's predicted function in ESCC within our study. Future investigations should aim to further classify LPXN's mechanism and cellular functions in ESCC. The relationship between ESCC, immune cell infiltration, and immune checkpoints offers novel insights into additional potential roles for LPXN in ESCC treatment, albeit necessitating further experimental verification. The factor of controversy surrounding the selection of suitable biological matrices for potential biomarker exploration, considering both tissue-based and liquid biopsy samples, presents as diffuse and broadly agreed-upon biological specimens for routine practice. Notwithstanding, a significant strength lies in the technical methodologies employed in identifying molecular alterations of LPXN. This study underscores LPXN's potential part in fostering cancer and its mechanism in ESCC development. Nevertheless, the prospect of utilizing LPXN as a tumor marker to forecast the disease remains uncertain. Its specificity, sensitivity, and the need for clinical detection kits mandate additional research.
{kind=link}