This meta-analysis has quantitatively examined the bidirectional relationship between tooth loss and hypertension. A total of 16 studies were included. There were about 177 ,000 participants in the pooled analysis of the incident hypertension among individuals with tooth loss and 7,600 participants in the pooled analysis of the incident tooth loss among individuals with hypertension.
The effectiveness of tooth loss as a predicator of incident hypertension
In general, there was no significant association between tooth loss and incidence of hypertension, no matter the number of tooth loss. As the included studies were all longitudinal, we confirmed that the result was credible. However, one study[19] showed that individuals who lost more than three natural teeth were more likely to develop hypertension compared to individuals lost less than three teeth. Firstly, the study was a cross-sectional study which couldn’t reveal the substantial sequence of tooth loss and hypertension. Secondly, the definition of exposure and comparator was different from other included studies which might result in the different result. Besides, we noticed that the result in the study varied with the number of lost teeth and stage of hypertension. Compared with individuals lost no more than three teeth, participants lost more than 15 teeth showed no significant difference in incidence of hypertension, which was partly consistent with our pooled analysis. Therefore, though several studies showed that tooth loss might act as a predictor for diabetes [28, 29] and metabolic syndrome[30], there is still no comprehensive evidence for the effectiveness of tooth loss as a predicator of incident hypertension. However, our result didn’t repudiate the possibility that after the number of tooth loss exceed a certain number, the incidence of hypertension might increase. It was reported that tooth loss was associated with increased blood pressure (not fit the criterion of hypertension) in adults[31]. More high-quality prospective cohort studies remained to be done to reveal the curve between the number of tooth loss and incident hypertension.
The risk of tooth loss among individuals with hypertension
Our result suggested that hypertension was significantly associated with incidence of tooth loss. Consistent with our study, a recent review showed that hypertension could predict tooth loss among patients with periodontitis[32]. Therefore, individuals with hypertension should pay more attention to the oral health. It was reported that long-term periodontal maintenance might improve the oral health and decrease the incidence of tooth loss [33], which might also apply to patients with hypertension. We noticed that there was no significant association between hypertension and incident edentulism, which was reported for the first time. Since the risk of tooth loss (except edentulism) increased among patients with hypertension, the risk of edentulism should increase, too. After discussion, we concluded that the diagnostic criterion of edentulism was much harder to be fit than other types of tooth loss which resulted in the relatively low incidence of being edentulous compared to tooth loss and might further contribute to the unexpected result. Besides, subgroup by study design showed that there was no significant association between hypertension and incident tooth loss according to longitudinal studies while among cross-sectional studies, the relationship was significant. Considering the drawback of cross-sectional study, we should be cautious about the result. More high-quality prospective studies remain to be done to reveal the substantial relationship between hypertension and tooth loss.
To obtain more clinically specific results, we conducted subgroup analysis by age, gender ratio and religion. According to our results, the OR between hypertension and incident tooth loss declined with age, and the significant association only existed among individuals no more than 65 years old. Epidemiology research showed that the prevalence of severe tooth loss increased gradually with age and reached a peak at about 65 years old [34]. We guess that older people might pay more attention to their oral health and care of teeth which might partly counteract the effect of hypertension on tooth loss. Besides, the incidence of other risk factors of tooth loss including diabetes [35] and metabolic syndrome [36] showed an increase with age which might reduce the correlation between hypertension and tooth loss. There was still no satisfied explanation for this problem and more work remained to be conducted.
Subgroup by gender ratio (female/male) suggested that hypertension was significantly associated with tooth loss in population of which female made up the majority. The similar result didn’t apply to population with gender ratio (female/male) < 1. It was the first time to be reported. Previous studies have suggested that smoking, diabetes and their combination with hypertension was associated with high risk of periodontitis [37, 38], which might further result in tooth loss [39]. To the best of our knowledge, males are more likely than females to smoke cigarette and develop diabetes [40, 41]. Therefore, the correlation between hypertension and incidence and tooth loss should be higher in male than female. We noticed that the heterogeneity was considerable in population with gender ratio (female/male) ≥1 which decrease the credibility of the result. Besides, the included studies with gender ratio (female/male) were all conducted in Japan which might cause the bias of the result.
Region-specific analysis showed different results in different regions. Hypertension was significantly associated with tooth loss only in Middle Asia but not in East Asia and North America. Both race and income level were reported to be associated with tooth loss [42, 43]. People with high income level tend to care more about their oral health which might reduce the incidence of tooth loss. Besides, the dietary patterns, smoking and alcohol consumption were all related to the oral health[44, 45]. All of these might contribute to the different results of the association between hypertension and incidence of tooth loss.
In conclusion, our result suggested that individuals with hypertension should pay more attention to their oral health to prevent excessive tooth loss, especially for people no more than 65 years old and Middle Asia.
4.3 Biological mechanisms
Increasing studies has been done to explore the potential mechanisms of tooth loss and hypertension. Basically, we concluded the following three aspects of common mechanisms for tooth loss and hypertension. Firstly, hypertension was reported to be associated with chronic inflammation. It has been demonstrated in numerous clinical trials that hypertensive patients commonly have increased plasma CRP levels [46-48]. Besides, studies have showed higher plasma IL-6, IL-1β, and TNF-α levels in hypertensive patients compared to normotensive patients[49]. All the inflammatory factors might promote the occurrence of periodontitis, and cause tooth loss. Secondly, hypertension was associated with vascular dysfunction and might result in arteriosclerosis and microcirculation disorders [50, 51], which might influence the blood supply of root of tooth, promote oral infection and result in tooth extraction. Lastly, patients with hypertension show a high risk of developing other chronic diseases, including diabetes, metabolic syndrome and coronary heart disease, all of which was reported to be associated with tooth loss[32, 52, 53]. Combined with these chronic diseases, hypertensive patients might experience an earlier and severer tooth loss.
Strengths and limitations
The strengths of our study are as follows. Firstly, the study was the first systematic analysis and meta-analysis focused on the bidirectional relationship between hypertension and tooth loss in the recent twenty years and we further discussed the effects of age, gender and religion on the association. Secondly, the quality of included longitudinal studies were moderate or high, which contributed to the high reliability. Thirdly, we systematically analyzed the bidirectional association between tooth loss and hypertension, which provided the new and comprehensive evidence for reducing the heavy burden of tooth loss.
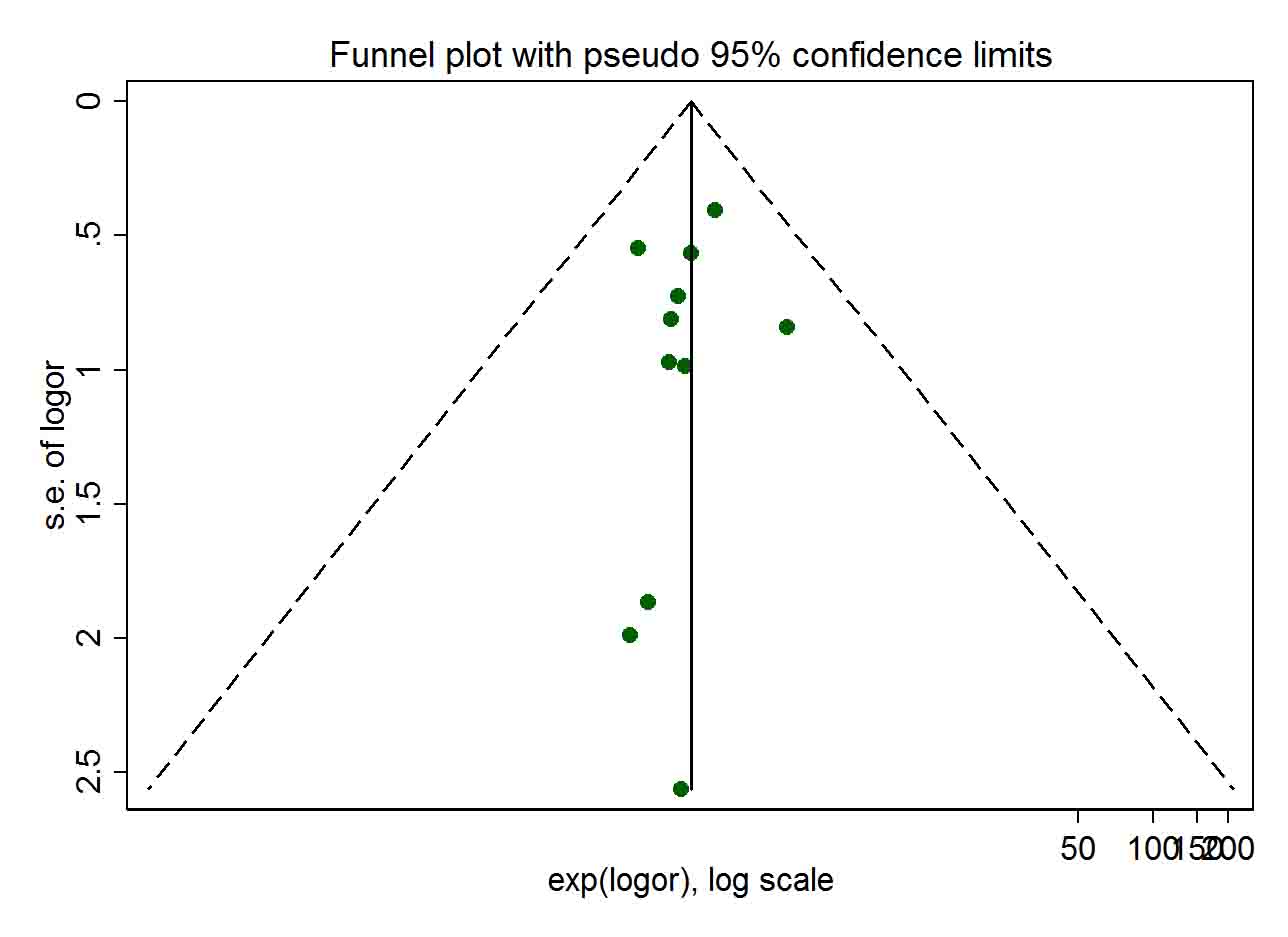
There were limitations of our study in the following aspects. Firstly, considering the limited number of longitudinal studies, cross-sectional studies were included in meta-analysis which might reduce the credibility of results and cause the defect of proving causality relationship. Secondly, the number of included studies is not enough, especially for subgroup-analysis. Thirdly, several pooled results showed a high heterogeneity while we failed to reduce it by extracting several studies. Fourthly, part of our included studies didn’t provide the OR with 95%CI that we needed for analysis so we calculate them by ourselves which might cause bias of the results. Besides, we failed to obtain the comprehensive curves of the number of lost teeth and the incidence of hypertension due to the lack of data. Lastly, diabetes, BMI, smoking status and other factors might also have an interaction with tooth loss and hypertension, which was not discussed in the study.
Recommendations for future research
Study design
We suggest high-quality prospective cohort studies with detailed baseline information and regular health examination as ideal study method. Population with different features including a specific job or different age groups and gender composition should be recorded and synthesized by stratified analysis. Smoking status, alcohol consumption, mental health, geographical region and other potential factors should be taken into consideration for the improvement of the representativeness.
The number of lost tooth
Future studies should record the number of teeth that participants lost and divide them into different groups. The association between tooth loss and hypertension need more quantification.
Adjustment by covariates
We found various covariates which may exert unstable impact on the summary during the review of eligible studies. We recommend standardized covariates should include at least age, gender, race, BMI, alcohol consumption, smoking status, health level in the baseline, socioeconomic status at an individual level. This work requires detailed and elaborate baseline information.
{kind=link}
{kind=link}