Overview of DA-CPR and BCPR (Fig. 1, lower part)
Unwitnessed cases (62.6%) had more frequent DA attempts than bystander-witnessed cases (52.3%) (unadjusted OR [95% CI]: 1.53 [1.50–1.55]). Regardless of DA provision, bystander-witnessed cases (72.4%, with DA; 32.0%, without DA) more frequently received BCPR than unwitnessed cases (65.7%, with DA; 23.9%, without DA) (1.39 [1.36–1.43] and 1.50 [1.46–1.53], respectively). In the groups with BCPR provision, unwitnessed cases (91.1%, with DA; 81.7%, without DA) more frequently received compression-only BCPR than bystander-witnessed cases (39.6%, with DA; 77.1%, without DA) regardless of DA attempts (1.37 [1.32–1.42] and 1.33 [1.26–1.40], respectively).
Beneficial effects of BCPR on outcomes
BCPR improved the overall outcomes, with a significant interaction with witness status (Table 1). The outcomes of bystander-witnessed cases were considerably better than those of unwitnessed cases. Thus, BCPR significantly improved the outcomes mainly in bystander-witnessed cases.
Table 1
Association of bystander CPR with outcomes of OHCA
| Characteristic and outcomes | Bystander CPR (Chest compressions with and without rescue breathing by bystanders) | Unadjusted OR (95% CI) with no bystander CPR as reference | Adjusted OR with no bystander CPR as reference a) |
| Not provided by bystanders | Provided by bystanders |
| All EMS-unwitnessed OHCAs (N = 329,923) | | | | |
| N | 160,957 | 168,966 | | |
| 1-M survival, % (N) | 3.9 (6,179) | 4.9 (8,214) | 1.28 (1.24–1.32) | 1.11 (1.06–1.15) b) |
| Neurologically favourable outcome, % (N) | 1.6 (2,605) | 2.5 (4,224) | 1.56 (1.48–1.64) | 1.23 (1.16–1.31) c) |
| Unwitnessed OHCAs (N = 212,003) | | | | |
| N | 105,851 | 106,152 | | |
| 1-M survival, % (N) | 1.8 (1,900) | 1.8 (1,858) | 0.97 (0.91–1.04) | 0.90 (0.64–1.28) |
| Neurologically favourable outcome, % (N) | 0.66 (694) | 0.65 (686) | 0.99 (0.89–1.10) | 1.13 (0.99–1.29) |
| Bystander-witnessed OHCAs (N = 117,920) | | | | |
| N | 55,106 | 62,814 | | |
| 1-M survival, % (N) | 7.8 (4,279) | 10.1 (6,356) | 1.34 (1.28–1.39) | 1.29 (1.21–1.38) |
| Neurologically favourable outcome, % (N) | 3.5 (1,911) | 5.6 (3,538) | 1.66 (1.57–1.76) | 1.46 (1.36–1.57) |
| OHCA: out-of-hospital cardiac arrest, CPR: cardiopulmonary resuscitation, OR: odds ratio, CI: confidence interval, DA-CPR: dispatcher-assisted CPR instruction. |
| a) Multiple variable regression analyses included the followings as candidate for the final model with the least Akaike Information Criterion: patient age, sex, emergency call during nighttime (10:00 p.m.–6:00 a.m.), bystander CPR (chest compressions), shockable initial rhythm, public access defibrillation, any prehospital defibrillation, presumed cardiac etiology, advanced airway management, tracheal intubation, classification of epinephrine administration (no epinephrine, early [EMS initiation of CPR-first administration < 13 min] single-dose administration and other administrations), and time intervals of emergency call-to-first CPR interval, call-to- EMS contact to patient and and EMS contact to patient-to-EMS arrival at hospital interval. In the analysis for all EMS-unwitnessed OHCAs, witness and its interaction with bystander CPR were also included. |
| b) Significant interaction between witness and bystander CPR (P < 0.01). adjusted OR; 95% CI with unwitnessed cases as reference: 3.02; 2.85–3.19. |
| c) Significant interaction between witness and bystander CPR (P < 0.01). adjusted OR; 95% CI with unwitnessed cases as reference: 2.76; 2.28–3.26. |
Comparisons of the outcomes of the four BCPR groups with those without BCPR in unwitnessed and bystander-witnessed cases
In unwitnessed cases, lower rates of neurologically favourable outcomes (0.52% vs 0.66%, adjusted OR [95% CI], 0.88 [0.76–1.01]) and lower 1-M survival rate (1.5% vs 1.8%, 0.89 [0.81–0.97]) were observed in compression-only BCPR with DA compared with those in no BCPR (Fig. 2A). The rates of neurologically favourable outcome and 1-M survival were highest in standard BCPR without DA (1.2% and 2.5%, respectively).
In bystander-witnessed cases, higher rates of neurologically favourable outcomes and 1-M survival were observed in all four BCPR groups compared with those without BCPR (Fig. 2B). The rates of neurologically favourable outcomes and 1-M survival were highest in standard BCPR with DA (6.6% and 10.9%, respectively).
Component analyses of the combination of rescue breaths and chest compressions and DA provision in OHCA cases receiving BCPR
When the characteristics of unwitnessed OHCA cases receiving BCPR were compared between groups with and without DA-CPR (Table 2, left part), the differences were remarkable (unadjusted OR of < 0.8 or > 1.25 for nominal variables and median value for continuous variables) in terms of age, PAD, any prehospital defibrillation, advanced airway management, ALS by physician and time interval between emergency call and first CPR. Cases with DA were younger and less frequently had PAD, prehospital defibrillation, advanced airway management and ALS by physician than those without DA. However, BCPR initiation was delayed in cases with DA.
Table 2
Association between clinical characteristics of BCPR and OHCA in unwitnessed cases with bystander CPR
| Clinical characteristics and outcomes | Characteristics of bystander CPR |
| DA-CPR | | Combination of ventilations with chest compressions in BCPR |
| BCPR with DA-CPR | BCPR without DA-CPR | Unadjusted OR (95% CI) with BCPR without DA-CPR as reference or P value | | Standard | Compression-only | Unadjusted OR (95% CI) with compression-only BCPR as reference or P value |
| N | 87,192 | 18,960 | | | 11,270 | 94,882 | |
| Male, % (N) | 51.6% (44,978) | 50.8% (9,627) | 1.03 (1.01–1.07) | | 45.5% (5,131) | 52.1% (49,474) | 0.77 (0.74–0.80) |
| Age, y, median (IQR) | 81 (70–87) | 82 (70–88) | < 0.01 | | 82 (70–88) | 81 (70–87) | < 0.01 |
| Emergency call during nighttime (10:00 p.m.–5:59 a.m.), % (N) | 21.9% (19,058) | 22.0% (4,162) | 0.99 (0.96–1.03) | | 21.4% (2,408) | 21.9% (20,812) | 0.97 (0.93–1.01) |
| Of presumed cardiac etiology, % (N) | 64.2% (55,978) | 62.6% (11,872) | 1.07 (1.04–1.11) | | 63.1% (7,113) | 64.0% (60,706) | 0.96 (0.92–1.08) |
| Shockable initial rhythm, % (N) | 3.1% (2,693) | 3.8% (718) | 0.81 (0.74–0.88) | | 3.7% (411) | 3.2% (3000) | 1.16 (1.04–1.29) |
| Any prehospital defibrillation, % (N) | 6.1% (5,324) | 8.2% (1,545) | 0.73 (0.69–0.78) | | 9.0% (1,018) | 6.2% (5,891) | 1.51 (1.41–1.62) |
| Public access defibrillation,% (N) | 0.9% (818) | 2.9% (557) | 0.31 (0.28–0.35) | | 3.7% (412) | 1.0% (963) | 3.70 (3.29–4.16) |
| Advanced airway management, % (N) | 42.7% (87,192) | 35.9% (18,960) | 1.33 (1.29–1.38) | | 40.9% (4,604) | 41.6% (39,470) | 0.97 (0.93–1.01) |
| Tracheal intubation, % (N) | 7.7% (6,673) | 7.5% (1,423) | 1.02 (0.96–1.08) | | 8.1% (912) | 7.6% (7,184) | 1.07 (1.00–1.15) |
| Prehospital epinephrine administration, % (N) | | | | | |
| No | 85.9% (74,912) | 86.8% (16,463) | < 0.01 | | 84.4% (9,512) | 86.3% (81,863) | < 0.01 |
| Early single administration | 2.3% (2,020) | 2.2% (422) | | | 2.9% (328) | 2.2% (2,114) | |
| Other administrations | 11.8% (2,075) | 10.9% (2,075) | | | 12.7% (1,430) | 11.5% (10,905) | |
| Physician in ambulance, % (N) | 2.4% (2,082) | 2.9% (555) | 0.81 (0.74–0.89) | | 3.6% (401) | 2.4% (2,236) | 1.53 (1.37–1.70) |
| ALS by physician, % (N) | 8.0% (6,970) | 10.6% (2,000) | 0.74 (0.70–0.78) | | 10.1% (1,138) | 8.3% (7,832) | 1.25 (1.17–1.33) |
| Time intervals, min, median (IQR) | | | | | |
| Emergency call-to-BCPR (first CPR) | 1 (0–2) | 0 (-2–2) | < 0.01 | | 0 (-3–1) | 1 (0–2) | < 0.01 |
| EMS response time interval | 9 (7–11) | 9 (7–11) | 0.85 | | 9 (7–11) | 9 (7–11) | 0.54 |
| EMS contact to patient-to-arrival at hospitals | 22 (17–28) | 22 (17–29) | < 0.01 | | 22 (17–28) | 22 (17–28) | 0.62 |
| OHCA: out-of-hospital cardiac arrest, CPR: cardiopulmonary resuscitation, OR: odds ratio, CI: confidence interval, BCPR: bystander CPR, DA-CPR: dispatcher-assisted CPR instruction, PAD: Public access defibrillation, EMS: emergency medical service, ALS: advanced life support. |
When the characteristics of unwitnessed OHCA cases receiving BCPR were compared between compression-only and standard BCPR groups (Table 2, right part), cases with compression-only BCPR were younger and less frequently had PAD, prehospital defibrillation and ALS in ambulance than those with standard BCPR. However, BCPR initiation was delayed in cases with compression-only BCPR.
Some characteristics of bystander-witnessed cases differed between the BCPR groups. Notably, the incidence of shockable rhythm in bystander-witnessed cases was higher in the groups receiving BCPR with DA and compression-only BCPR, whereas that in unwitnessed cases was slightly higher in the groups receiving BCPR without DA and standard BCPR (Supplementary Table 1).
According to simple binominal logit analyses with interaction test, BCPR with DA was associated with less neurologically favourable outcome and worse 1-M survival in unwitnessed cases; meanwhile, standard BCPR was associated with better outcomes in both unwitnessed and bystander-witnessed cases receiving BCPR (Table 3). A significant interaction was found between DA provision and standard BCPR for 1-M survival in unwitnessed cases (P = 0.01) and for neurologically favourable outcomes in bystander-witnessed cases (P = 0.01).
Table 3
Associations of clinical characteristics of bystander CPR with outcomes of OHCA (Simple binominal logit analysis with interaction test)
| Outcomes of OHCA | Characteristics of bystander CPR | Interaction of the two bystander CPR characteristics |
| DA-CPR | | | Combination of rescue breaths with chest compressions in BCPR | |
| BCPR with DA-CPR | BCPR without DA-CPR | Adjusted OR (95% CI) with BCPR without DA-CPR as reference | | Standard | Compression-only | Adjusted OR (95% CI) with Compression-only BCPR as reference |
| Unwitnessed OHCA | | | | | | | | |
| N | 18,960 | 87,192 | | | 11,270 | 94,882 | | |
| 1-M survival | 1.6% (1,406) | 2.4% (452) | 0.78 (0.68–0.90) | | 2.4% (274) | 1.7% (1,584) | 1.30 (1.13–1.50) | P = 0.01 |
| Neurologically favorable outcome | 0.56% (484) | 1.1% (202) | 0.61 (0.49–0.76) | | 0.98% (110) | 0.61% (576) | 1.39 (1.12–1.72) | P = 0.07 |
| Witnessed OHCA | | | | | | | | |
| N | 44,832 | 17,982 | | | 9,422 | 53,392 | | |
| 1-M survival, % (N) | 10.1% (4,525) | 10.2% (1,831) | 1.01 (0.94–1.09) | | 10.8% (1,017) | 10.0% (5,339) | 1.08 (1.01–1.17) | P = 0.61 |
| Neurologically favorable outcome, % (N) | 5.5% (2,467) | 6.0% (1,071) | 1.00 (0.91–1.10) | | 6.3% (595) | 5.5% (2,943) | 1.11 (1.01–1.22) | P = 0.01 |
| OHCA: out-of-hospital cardiac arrest, CPR: cardiopulmonary resuscitation, OR: odds ratio, CI: confidence interval, BCPR: bystander CPR, DA-CPR: dispatcher-assisted CPR instruction. Adjusted OR was calculated by binominal analysis including DA-CPR and combination of rescue breaths with chest compressions in BCPR. |
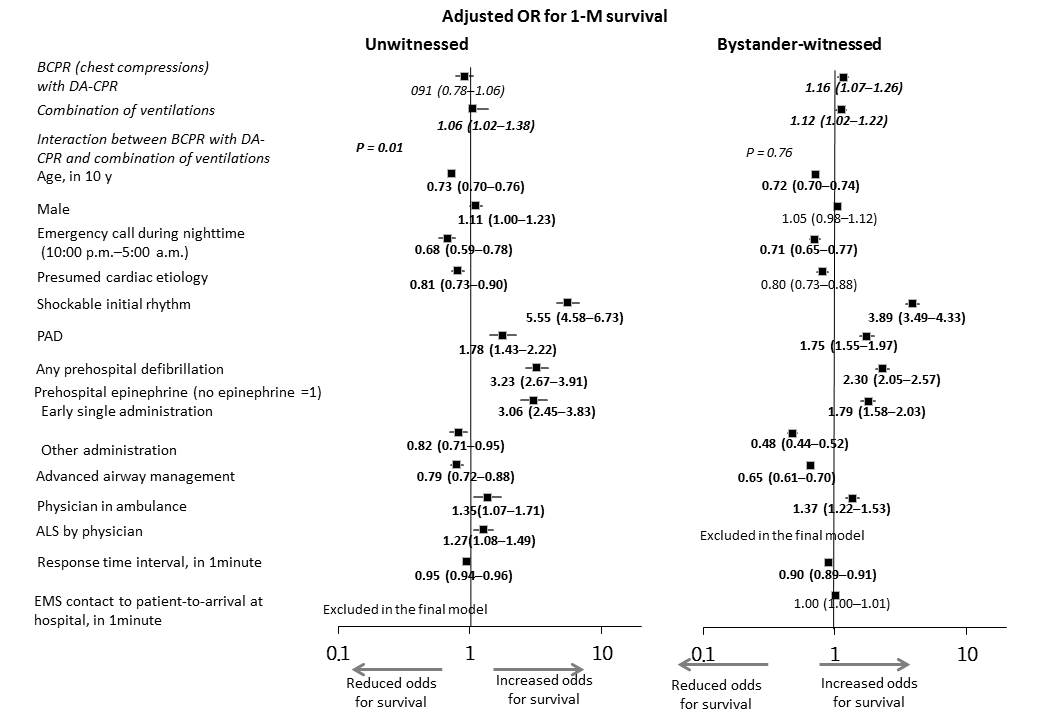
Multivariable analysis on neurologically favourable outcomes (Fig. 3) revealed that BCPR with DA was associated with worse outcomes in unwitnessed cases (adjusted OR [95% CI], 0.76 [0.60–0.97]) and better outcomes in bystander-witnessed cases (1.28 [1.14–1.43]). This Fig. is particularly helpful in getting an at-a-glance summary. However, standard BCPR was associated with better outcomes only in unwitnessed cases (1.27 [1.01–1.60]). Regarding 1-M survival, standard BCPR was associated with higher survival rates in both unwitnessed cases (1.06 [1.02–1.38]) and bystander-witnessed cases (1.16 [1.07–1.26]). However, DA was associated with higher survival rates (1.16 [1.07–1.26]) only in bystander-witnessed cases (Supplementary Fig. 1). Other major common factors associated with neurologically favourable outcomes were age, initial shockable rhythm, any prehospital defibrillation and response time interval. Notably, early single administration of epinephrine was associated with a higher 1-M survival rate but not with better neurologically favourable outcomes.
{kind=link}