When we fixed the bone flap with metal wire or suture thread such as silk or nylon, the fixation was not enough and some problems often happened.[3, 9] The osteofixation of titanium plate have been developed. Titanium plates are able to fix a bone flap easily but also rigidly. Thus, titanium plates are now widely used at craniotomy. However, adverse events associated with titanium plates are reported especially for pediatric case implanted for a long period. It is reported that deviation of the plates, inhibition of cranial bone growth, aberrance into brain, scalp thinning and plates exposure.[6, 7, 9, 13, 18]
Recently, Various bioresorbable osteofixation implant materials have been developed. It have been reported that polyhydroxyl acids, poly-D-lactic acid, polyglycolic acid, etc. as materials. The first use of bioresorbable implants to animals was published in 1966 by Kulkarni et al. [10] Bioresorbable materials are inferior to titanium in terms of fixing strength, but have same biocompatibility as titanium. Several reports described that adverse effects were no difference between bioresorbable and titanium materials, so bioresorbable materials are not inferior to the titanium materials.[1–3, 8, 12, 20]
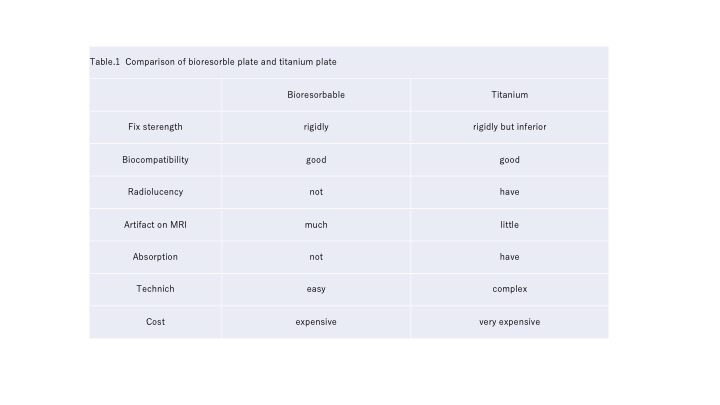
Bioresorbable materials are absorbed in about a year, eliminating the need to remove the implant after osseous healing. And bioabsorbable materials benefit from reduced tactile sensation, pain, and radiolucency. (Table 1).[4, 9, 17] Because of those advantages described above, the use of them for pediatric cases have been increasing.
Our case showed the fracture of bioresorbable plates after head injury. Lactosorb® which we used in this case, is made from a copolymer of 82% poly-L-lactic acid and 18% polyglycolic acid. In vitro exposure, it is reported that it retains about 70% of initial shear strength after 8 weeks. Thus, it is considered that Lactosorb® fix strength has retained until natural osseous healing.[11, 15, 19] The times of resorption of the copolymer plate is about a year.[13] The screws made of the same material has about 80% of initial shear strength at four weeks and keeps the strength after that.[16] It is also reported that bioresorbable plate has similarly bending and tensile stiffness as titanium plate but showed low side bending stiffness.[14]
APACERAM® which we used as bone flap at cranioplasty is made from microporous hydroxyapatite. Newly formed bone was detected on the surface of the material and in the macropores near the surface 1 week after transplantation, and it was reported that the compressive strength of 10 MPa is maintained after 5 weeks.[19]
This case was injured 8 weeks after the cranioplasty, and was thought to have been about 70% of the initial shear strength of the plate at that time. In this case, it was probable that the bone flap sank due to head injury and the bioabsorbable plate was subjected to lateral bending stress, resulting in division at the central part. As a result, the dura mater was injured by the edge of the bone flap and occurred the cerebrospinal fluid leakage and made the skin bulging.
By the time the bioabsorbable plate was absorbed, it is thought that bone healing and adhesion to peripheral bone would progress and shear strength would be maintained. In this case, the bioabsorbable plate was damaged by a head injury before such a condition occurred. This case indicated that it is necessary to pay much attention to early head injury after cranioplasty with bioresorbable plates.
{kind=link}