Unilateral pulmonary artery discontinuity (UPAD) is a rare congenital heart disease (CHD) with an estimated prevalence of 1 in 200,000 people1 and initially described by Fraentzel, 1868.3 It is also referred to as isolated unilateral pulmonary artery agenesis or ductal origin of distal pulmonary artery(DODPA), the former one term can be misleading as an intrapulmonary vessel is present in fetuses with this condition. UPAD is more widely accepted and used, as it clarifies that that the proximal pulmonary artery discontinuity and the distal part still exist. Embryologically, under normal conditions the proximal sixth aortic arch will form extrapulmonary pulmonary artery and join intrapulmonary pulmonary arteries. The majority of UPAD studies have indicated that the cause of this developmental defect is the involution of the proximal sixth aortic arch, resulting in the absence of extrapulmonary pulmonary artery.4 Consequently, a single pulmonary artery arising from the main pulmonary artery (MPA) trunk can be picked up on ultrasound imaging, while the intrapulmonary pulmonary arteries arise from their respective lung buds normally and persistently connect with the distal sixth aortic arch. This explains why, during ultrasound scanning from the hilum, the distal segment of the pulmonary artery is normally connected to the corresponding lung tissue. Since the distal sixth aortic arch destine to become the ductus arteriosus, the pulmonary artery always arise by way of ductus-like collateral vessels from the aortic arch system or from bronchial arteries. In our case, the pulmonary artery originated from the descending aortic arch through the ductus arteriosus.
Accurately determining the origination of the pulmonary artery from what part of aorta is crucial. If the unilateral pulmonary artery anomaly originates from the ascending aorta, it is classified as hemitruncus arteriosus5 or anomalous origin of one pulmonary artery from the ascending aorta (AOPA). In comparison to UPAD, these anomalies typically result in life-threatening pulmonary hypertension earlier due to the pulmonary artery with anomalous origin receives disordered and high-pressure blood perfusion from the aorta, while another pulmonary artery receives perfusion from the whole right ventricle. According to the distance between the anomalous origin of the pulmonary artery and the aortic valve, it can be classified into proximal and distal types. Distinguishing the distal-type from UPAD on ultrasound is challenging.
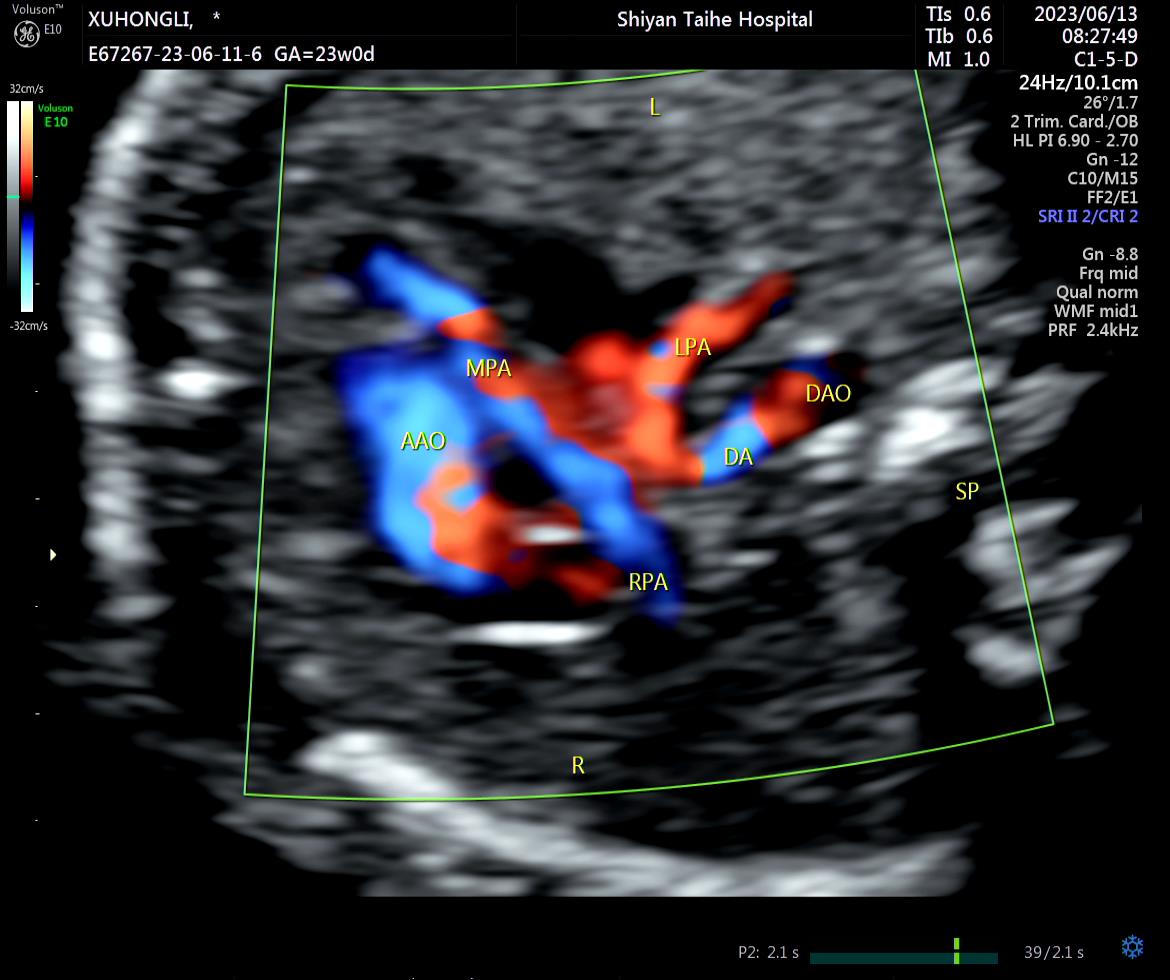
UPAD is mostly coexist with other CHD but can also present as an isolated anomaly. The occurrence of left pulmonary artery discontinuity (LPAD) in conjunction with other CHDs is more prevalent compared to the right pulmonary artery, such as Tetralogy of Fallot (TOF), septal defect, persistent ductus arteriosus (DA), or mirror image right aortic arch(MRAA).6,7 Nevertheless, rare literature documents the prenatal echocardiographic diagnosis of the left pulmonary artery originating from the ductus arteriosus coexist Taussig-Bing syndrome. The most commonly association of LPAD is TOF5, which can be easily confused in imaging with Taussig-Bing syndrome. In our case, ultrasound should be employed for the identification of Taussig-Bing syndrome. this syndrome is characterized by an overriding pulmonary artery across a ventricular septal defect (VSD), a complete transposition of the aorta originating solely from the right ventricle, bilateral subarterial conus with an absence of pulmonary-mitral fibrous continuity, and side-by-side great vessels can be found.8
In the prenatal stage, Isolated unilateral pulmonary discontinuity can be difficult to diagnose, as its early symptoms are not obvious. However, after birth, if the ductus arteriosus closes or there is vascular endothelial injury, symptoms such as coughing, hemoptysis, and recurrent respiratory infections may arise, which can potentially pose a threat to life9.
Summarizing the previous experience, there is a consensus among sonographers performing fetal malformation screening that conducting a continuous scan enables the acquisition of more comprehensive anatomical information10. In challenging cases where identification of the ipsilateral pulmonary artery origin proves difficult, it is recommended to perform upstream scanning from the hilum to locate its origin and course. Furthermore, in our study, we utilized spectral Doppler ultrasound to measure the spectrum of pulmonary arteries on both sides and observed similar waveforms. Therefore, spectral Doppler can be a valuable tool for assisting in the diagnosis of undiagnosed ( but suspected) abnormal origin vessels. Identifying the origin of the pulmonary artery should be considered routine prenatal screening to prevent missed detection of various anomalous origins such as Anomalous Origin of Pulmonary Arteries (AOPA), Pulmonary Artery Sling, Crossed Pulmonary Arteries (CPA), among others that are often challenging to identify using conventional views. Currently new technology provides better support for diagnosis, for example L. Chen et al11 uses the STIC-HD (four-dimensional spatiotemporal image correlation) live flow technology to acquire the overall perspective of all blood vessels, which can help physicians to have new visual experiences of clear depiction of fetal great vessels.
Over the past decade, The frequency of intrauterine detection of UPAD has been gradually increasing. However, it is more commonly detected in children and young adults due to clinical symptoms rather than prenatal diagnosis.2,12 We conducted a comprehensive analysis of the existing English literature on fetal UPAD identified in PubMed within the past decade. The available research encompassed merely five studies, comprising a total of sixteen documented cases. Table 1 provides the information about each case report. From the data in Table 1, it can be observed that 5 (30%) out of 17 patients had isolated UPAD with no other cardiac malformations. Additionally, in 12 (70%) cases, UPAD was associated with other congenital heart diseases, most commonly ventricular septal defect (n = 6), followed by mirror image right aortic arch (n = 4), double-outlet right ventricle (n = 2), tetralogy of Fallot (n = 1), Taussig-Bing syndrome (n = 1),and persistent left superior vena cava (n = 1). In this group, Isolated RPAD is less common than LPAD with CHD, accounting for 30% of all cases. Among the 10 LPAD cases, 6 (60%) were not associated with MRAA, which contradicts the finding of Li et al13 that the proximal pulmonary artery was found to be absent on the contralateral side of the aortic arch.However, it is worth noting that MRAA was never found in cases of RPAD. Isolated RPAD accounted for approximately 70% of all RPAD cases, and only 2 cases of RPAD were associated with other CHD, namely a small ventricular defect and PLSVC.
Table 1
Prenatal ultrasonographic manifestations and follow - up results of 17 cases of Unilateral pulmonary artery discontinuity
| Years | Author | Case | Gestational ago(weeks) | Affected PA | Associated heart anomalies | Outcome |
| 2022 | L. Chen11 | 1 | 25+ 3 | RPA | None | Full-term delivery, surgery, alive |
| | | 2 | 23 | LPA | MRAA | TOP,confirm end by autopsy |
| | | 3 | 24 | RPA | VSD | Full-term delivery, surgery,alive |
| 2021 | Hyun‑Hwa Cha14 | 4 | 26 | LPA | PA,VSD | Full-term delivery, surgery(RVOT reconstruction and pulmonary artery reimplantation),died(right heart failure) |
| 2020 | Li Wenxiu13 | 5 | 27 | RPA | None | Full-term delivery, PDO, alive |
| | | 6 | 28 | RPA | None | TOP, confirmed by autopsy |
| | | 7 | 25 | RPA | None | Full-term delivery, without surgery |
| | | 8 | 25 | RPA | None | Full-term delivery, without surgery |
| | | 9 | 25 | LPA | MRAA | Full-term delivery, without surgery |
| | | 10 | 26 | LPA | TOF, MRAA | Full-term delivery, TOF surgery, alive |
| 2018 | JianchengHan2 | 11 | 22+ 2 | RPA | PLSVC | TOP, confirmed by vascular casting |
| | Li Xuelei15 | 12 | 24 | LPA | RIM,SV pulmonary artery, IVC and LHV connected to the left atrium, MHV and DV and RHV connected to the right atrium | prenatal magnetic resonance imaging, TOP, confirmed by autopsy |
| | | 13 | 27+ 1 | LPA | PS, MRAA, sinistrocardia | TOP, confirmed by autopsy |
| | | 14 | 24+ 3 | LPA | SA, VSD, DORV, PS | TOP, confirmed by autopsy |
| | | 15 | 22+ 2 | LPA | VSD, DORV, PS | TOP, confirmed by autopsy |
| | | 16 | 23+ 2 | LPA | PA, VSD, | TOP, confirmed by autopsy |
| Current | Yun He | 17 | 23 | LPA | Taussig-Bing syndrome | TOP, confirmed by autopsy |
| Only first author of each study is given. |
| TOP, termination of pregnancy;VSD, ventricular septal defect;PA, pulmonary atresia;DORV, double-outlet right ventricle; PDO, patent ductus arteriosus occlusion; PLSVC, persistent left superior vena cava;MRAA,mirror image right aortic arch; RVOT, right ventricular outflow tract;SV, single ventricle; PS, pulmonary artery stenosis; SA, single atrium;atrioventricular septal defect; RIM, Right isomerism; IVC, Inferior vena cava; LHV, left hepatic vein; MHV, middle hepatic vein; RHV, right hepatic vein; DV, ductus venosus; |
UPAD refers to the involution of the sixth aortic arch resulting in discontinuity between the proximal and distal pulmonary arteries, along with a ductal origin of distal pulmonary artery. LPAD often coexist with complex congenital heart defects, while RPAD can be easily overlooked during routine scans. Therefore, whether managing complex CHD or conducting regular antenatal examinations, assessing the branching relationship of the pulmonary arteries through a three-vessel view becomes essential for identifying any abnormalities in their origins. Ultrasound is the preferred method for antenatal examination, aiming for more accurate and early detection of lesions. However, achieving this requires sonographers to possess a deeper understanding of basic views and a broader comprehension of diseases. This case emphasizes the importance of paying attention to the continuity of pulmonary arteries in detecting CHD, which significantly aids later-stage treatment. Furthermore, it reminder that LPAD can coexist Taussig-Bing syndrome equally.
{kind=link}