We used a qualitative iterative methodology, triangulating data from three different sources to facilitate a rich understanding of the barriers and facilitators of participation in research from patient and public perspectives:
-
Scoping review of current literature to identify studies relating to inclusive research, whose findings could be extrapolated beyond the individual study.
-
Two focus groups: with a PPIG; and with community leaders from four voluntary care organisations serving Roma, South Asian, Black, and socio-economically deprived populations of South Yorkshire to discuss their perspectives on ‘inclusive research’.
We consulted a variety of stakeholders in the design of the focus group/interview questions, including frontline practitioners, academics, and patients, and in the analysis stage, members of our research group (EL and JW)
Scoping review
A scoping review was undertaken to find and describe studies which identify transferable learning about doing research with under-served communities. The study design is based on Arksey and O′Malley’s Scoping Review Framework (11). It is reported according to Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) (12).
We will search for studies which are relevant to the UK context, which have sought to include underserved groups in research, and have findings with explicit transferable learning (ETL).
The search strategy was developed by KF and IH with input from the research team and carried out in Medline.
-
(Research adj3 (participat* or involve*))
-
(Underserved or "ethnic min*" or BAME or depriv*)
-
1 and 2
-
Cultur*
-
3 and 4
Titles were filtered by the researchers (KF, IH) independently. Studies were eliminated if titles indicated that they were not related to the process of research or not relevant to the UK context. The researchers then met to discuss discrepancies. Where agreement could not be reached, the study was included in the next stage.
Abstracts were reviewed for the remaining references, and eliminated if they were not applicable to the UK context and/or study specific with no explicit transferable learning (ETL). If this could not be determined by the abstract, the researchers referred to the full text.
Focus groups (setting and participants)
Focus groups were chosen to collect data as they are a well-accepted method in social science and the group process allows participants to identify and clarify their views (6). Potential participants were purposively sampled via a PPIG and community organisations serving ethnic minority and socio-economically deprived populations. They were contacted via email with a brief description of the research, and asked to contact the researcher (KF) if they would like to take part. They were then sent an information sheet with the opportunity to contact the researcher to ask questions, before returning a signed consent form.
The topic guide for focus group 1 (see appendix 1) was developed using the scoping literature review, NIHR’s INCLUDE (4) recommendations and insights, and stakeholder consultation.
Both focus groups were facilitated by KF. KF is a female post-doctoral Research Associate, with over 20 year’s experience of qualitative health research, including conducting focus groups and interviews. KF is white British, and a practising Muslim.
In the first focus group, 6 participants were recruited, with informed consent, from the PPIG. The participants were 2 men and 4 women, age between 40 and 75. 3 participants were White British, 1 Black African and 2 South Asian. All live in socio-economically deprived neighbourhoods (IMD index of multiple deprivation most deprived decile) .
A focus group lasting 75 minutes was conducted in a University building, which was easily accessible by both car and public transport. It was audio-recorded, transcribed verbatim, and then anonymised for analysis. KF took field notes to supplement the analysis.
Researchers (KF/JW/EL) undertook rapid thematic analysis (13) and created a template from the transcript to establish the key themes. This template was presented at the second focus group of community leaders. Template analysis involves the development of a coding ‘template’, which summarises themes identified by the researcher(s) as important in a data set, and organises them in a meaningful and useful manner (14).
For the second focus group, 4 community leaders were recruited from 4 community organisations, to represent a variety of underserved communities (Roma, South Asian, Black, and socio-economically deprived). The aims of the research were discussed with the participants when inviting them to the focus group. All who were invited, agreed to take part. The participants were 3 women and 1 man, ranging from age 40–70, and their ethnic backgrounds were Roma, South Asian, Black and White British.
KF had previously established professional relationships with these participants. The focus group took place online, as this was preference of the community leaders. The researcher (KF) and the participants were the only people in the meetings. One community leader was unable to attend on the day so was interviewed in a separate video call, following the same format. The focus group was 69 minutes long, and the interview was 40 minutes long. KF took field notes to supplement the analysis.
Community leaders were asked about social and cultural issues relating to their communities, and specific examples were drawn from the first focus group, with regard to perceptions of research, and barriers and facilitators to getting involved. Participants were also asked how academics and clinicians may be able to work with community groups to increase participation.
Three researchers (KF, JW, IH) conducting rapid thematic analysis of the focus group, further developed the template, which was then refined with the main research team (KF, CM, EL).
KF continually checked her understanding of what was being said in the focus groups with the participants, which was decided as preferable to sharing the transcript of the focus group afterwards, which would have been extremely time consuming for the attendees to read through.
The focus groups did not aim to reach data saturation, but to gather enough data from a variety of perspectives to provide conceptual depth, alongside the scoping review.
Analysis- an iterative triangulation of source data
Data extracted from papers identified in the literature review were thematically analysed (14) by two researchers (KF and IL).
Focus groups and the interview were analysed using Template Analysis (13) which involves developing a coding template, which is then applied and revised. The template was derived from discussions with clinicians in the research team, around the barriers and facilitators to involvement in research.
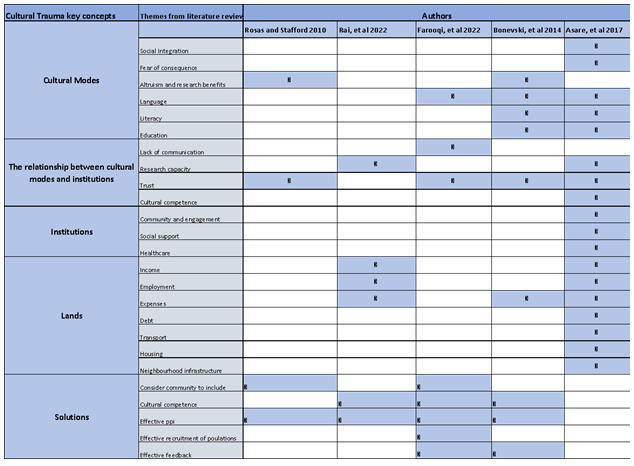
The template was then further developed from the 2nd focus group. Service level motivators were added in based on discussions with clinicians in the research team (see Fig. 1).
Figure 1 – Template Analysis
The focus groups and interview were then analysed according to this template. The final model was presented to the DEPPIG, who confirmed their views were adequately represented and the model made sense to them.
{kind=link}