Increased oxidative/nitrosative stress might play a major role in the progression of various lung diseases including AE-ILDs and ARDS (9-14). HO-1, a rate-limiting enzyme in heme catabolism, has antioxidative activities in patients with these diseases (27-29). We previously investigated whether evaluating the degree of oxidative stress by measuring serum HO-1 using the sandwich ELISA method is useful for assessing disease activities and predicting prognosis in patients with ARDS and AE-ILDs (19, 20). In the present study which was an integrated analysis of these previous studies, we investigated whether composite parameters including serum HO-1 and other clinical parameters could predict the prognosis of ARDS and AE-ILDs more accurately than serum HO-1 alone and oxidative stress measured by serum HO-1 levels could be reduced in the clinical course.
ARDS and AE-ILDs are a life-threatening event and the mortality rate is high (30, 31). A retrospective analysis in patients with ARDS showed a significant increase in hospital mortality in patients with DAD compared to those without DAD (71.9% vs 45.5%) (30). Other retrospective cohort study in patients with AE of chronic fibrosing interstitial pneumonia showed the overall survival after admission was 67% at 1 month and 40% at 3 months (31). In both patients with ARDS and AE-ILDs, our data showed better prognosis than these cohort studies, however, the patients with ARDS tended to show worse prognosis than those with AE-ILDs as previously reported. In the present study, ARDS patients had significantly higher serum HO-1 and CRP levels at baseline compared with AE-ILD patients and serum HO-1 had positive correlation with serum LDH. These results indicate that ARDS patients had a stronger degree of systemic inflammatory response, pulmonary epithelial cell damage and endothelial cell damage with the consequent increase of vascular permeability reflecting oxidative/nitrosative stress response than AE-ILD patients (32-34). Though similar with HO-1, SODs, catalase, and GPx had been described as the endogenous antioxidants, HO-1 characterized as stress response protein with relatively small-molecular weight (32 kDa, much smaller than KL-6 (5000 kDa)), rapid response against stimuli, and various physiological activities including the antiapoptotic, anti-inflammatory, vasodilatory, anticoagulant, antioxidant, and antiproliferative reactions caused by HO-1 metabolites (7, 15-17). Therefore, we speculate that serum HO-1 reflects pulmonary cellular damage induced by ROS and RNS more closely and directly.
Ongoing and persistent oxidative stress leads to poor prognosis (35). In patients with ILDs, persistently high ethane levels, a product of lipid peroxidation that has been proposed as a biomarker of oxidative stress, may correlate with poor prognosis (35). Cancer cells with persistent Nrf2 activation often develop Nrf2 addiction and show malignant phenotypes, leading to poor prognoses (36). In the present study, although serum HO-1 levels tended to decrease 2 weeks after the start of treatment in both ARDS and AE-ILD patients, serum HO-1 levels remained persistently high. Furthermore, in patients treated with intravenous corticosteroids, no significant decrease of serum HO-1 levels was observed. Systemic corticosteroids are able to block nuclear translocation of nuclear factor- kB, the main pathway of inflammatory cytokine synthesis, through their interaction with the glucocorticoid receptor, however, the use of corticosteroid in ARDS is not recommended routinely (37, 38). Also, retrospective data derived from AE-IPF patients treated with corticosteroid alone did not show any reduction in mortality rate over the short term (39). Several evidence in the animal models suggest that corticosteroid exposure can cause to increase oxidative stress (40, 41). Although the exact mechanism by which corticosteroid increase oxidative stress is not well known. several hypothesis have been reported that glucocorticoids could bind to mitochondrial glucocorticoid receptors and activate mitochondrial function to generate ROS or ROS is generated by the activation of the protein kinase C (PKC) β / p66shc signaling pathway by glucocorticoid in the cell (40, 41). Therefore, in patients with ARDS and AE-ILDs, the use of corticosteroids may be harmful from the point of view of oxidative stress increase, and the potential antioxidant treatment such as N-acetylcysteine needs to be examined in the future (42).
Composite approaches have been developed using peripheral blood biomarkers and physiological and radiographic measurements to provide more accurate prognostic information (26, 43, 44). For example, APACHE II score is frequently used to measure disease severity in intensive care unit patients with ARDS (26). The composite scoring system, which is based on serum LDH, Krebs von den Lungen-6, P/F ratio, and extent of abnormal high resolution computed tomography findings, is useful for predicting 3-month mortality in AE-IPF patients (43). We previously demonstrated that the Charlson Comorbidity Index score, sex, and serum LDH are important for predicting 3-month mortality in AE-ILD patients (44). In the present study, we found that composite parameters including serum HO-1, P/F ratio, sex, and age which was characterised as objective biomarkers had acceptable AUC for prediction of 3-month mortality in ARDS and AE-ILD patients. Our data suggest that composite parameters including serum HO-1 and other clinical parameters could predict the prognosis of ARDS and AE-ILDs more accurately than serum HO-1 alone. To verify the utility and reproducibility of this composite parameters, large-scale, multi-institutional prospective collaborative research is essential.
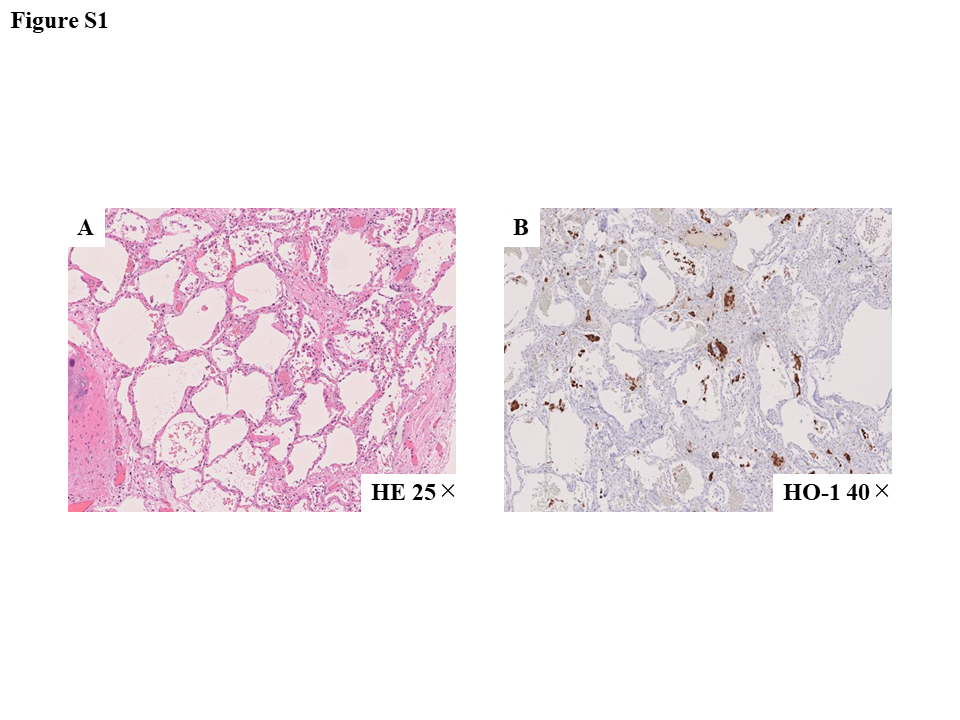
There are several limitations to the present study. First, the study enrolled only a small number of patients from a few institutions. Our findings need to be confirmed in a multi-centre, prospective study. Second, the various endogenous oxidative stress markers such as not only HO-1 but also SODs, catalase, GPx, and myeloperoxidase have been reported. It is necessary to evaluate which markers are the most reliable for predicting the prognosis of ARDS and AE-ILDs. Third, clinical diagnoses among ARDS and AE-ILD patients were heterogeneous. Actually, in both patients with ARDS and AE-ILDs, our data showed better prognosis than the previously reported cohort data. In the future, it is necessary to evaluate the clinical significance of serum HO-1 in patients with DAD histologically.


{kind=link}
{kind=link}
{kind=link}