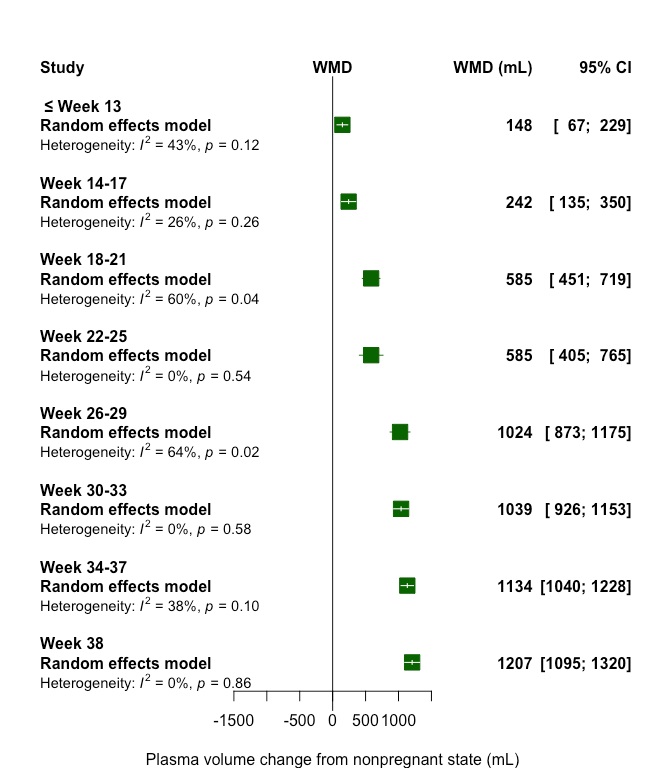
The current paper reviewed and synthesized studies with repeated measures of plasma volume from the same group of women with healthy pregnancies. Overall, 10 observational, longitudinal studies (347 total women) examining plasma volume changes across gestation in comparison to nonpregnant values were included in the meta-analysis. Based on this limited data, plasma volume increased to a small but measureable extent in the first trimester, followed by a sharp rise in the second trimester and a continuous but slow increase in the third trimester. The maximum weighted mean increase was 48% (1150 mL) above the nonpregnant volume, yet mean increases (percentage and/or volume) and the gestational age at peak expansion varied between studies.
Hytten was dedicated to understanding changes during normal pregnancy and reviewed studies of plasma volume in several publications including in his book “The Physiology of Human Pregnancy” [46] and a later review paper in Clinics in Haematology [47]. He did not use formal meta-analysis, but in compiling the few available studies, concluded that plasma volume expanded by just under 50% (1250 mL) among healthy women of European decent [47]. The range of normal plasma volume expansion was not provided for the first and second trimesters, nor the range of expansion around the 50% estimate. He acknowledged many factors that appear to influence baseline plasma volume and expansion during pregnancy, including maternal size, parity, and multiple gestation; these factors have been documented by Hytten and others [48]. While the available longitudinal data did not allow for stratification by these maternal factors, our meta-analysis estimate of a 48% maximum expansion was similar to Hytten’s estimate over 30 years ago.
Since the 1980s, there has continued to be a small amount of research on plasma volume. A recent review and meta-analysis combined studies from 1934 to 2007 to estimate plasma volume at gestational intervals across pregnancy compared to nonpregnancy [32]. Particularly informative, the authors compared plasma volume changes between healthy pregnancies and pregnancies with adverse outcomes such as preeclampsia, and found that expansion was lower in pregnancies with poor outcomes compared to healthy outcomes (32% vs. 46%). This was a comprehensive analysis, but unlike the current review, cross-sectional studies were included. Two concerns arise in using cross-sectional data to establish normal plasma volume expansion: 1) values during pregnancy and outside of pregnancy may be quite different for different women (see factors noted above) and 2) expansion is a change within an individual which inherently requires longitudinal data. Nevertheless, our estimates of maximum plasma volume expansion and the pattern of plasma volume expansion are similar to the expansion and pattern reported for healthy women in the de Haas et al. meta-analysis [32], showing consistency of findings across study designs.
Most studies reporting plasma volume expansion during pregnancy rely on a small number of women, few measurements, and minimal data reporting, making it difficult to know what is normal for aspects such as the range of volumes at peak expansion, the range of gestational ages at peak expansion, and the pattern of change beginning from periconception. Furthermore, we know even less about how these factors may differ across maternal characteristics such as weight, parity, age, and race/ethnicity. Still largely unknown is the degree of variability across different women with healthy pregnancies. The range of normal plasma volume expansion in healthy pregnancies has been reported as 25 to 80% [14] and 43 to 78% [49], but in general is rarely provided in publications. There may be a wide range in the gestational age at which women reach peak plasma volume (and whether or not it is maintained or slightly declines until delivery), and some studies have reported that women can reach peak volume as early as the second trimester [13, 42, 50]. Many aspects of volume and expansion are not uniformly reported in studies. The physiological mechanism responsible for plasma volume expansion during pregnancy are reviewed elsewhere [51, 52]. Briefly, it is thought that the activation of the renin-angiotensin-aldosterone system drives the rise in plasma volume during pregnancy.
Knowledge of the normal trend in plasma volume expansion, and the ability to measure it in clinical settings, is important because plasma volume expansion is a critical change in pregnancy needed for blood flow to the uterus, and it is associated with many health conditions. Low plasma volume is associated with an increased risk of developing gestational hypertension compared to normal plasma volume [4]. Furthermore, low pre-pregnancy plasma volume has been associated with recurrent preeclampsia, recurrent pregnancy loss, and risk of preterm delivery [5, 53]. Plasma volume may also affect biomarker concentrations. Biomarkers are important for clinical care, public health surveillance, and research alike. Some nutritional status biomarkers like vitamin B6, folate, zinc, copper, and hemoglobin have all been shown to change across gestation; the role of plasma volume in these changes has not been well described except for hemoglobin (creating lower cutoffs to diagnose anemia in pregnancy) [17, 54]. It is important to understand what level of changes in biomarkers are physiological and at what level of change should intervention be given to improve maternal and birth outcomes. Concurrently measuring plasma volume and nutritional biomarkers may be needed to understand these relationships.
Most of the studies available for this review were done in the 1960s and 1970s, a period when pregnant women were generally younger and leaner than those today [55-60]. It is unclear if the same pattern of expansion would be observed for older pregnant women [61], and maternal age during pregnancy has been continuing to rise in the US [62, 63]. Similarly, the prevalence of prepregnancy overweight and obesity has increased dramatically since the 1990s [55, 56, 58, 59]. It is likely that BMI could impact plasma volume [64], but the available studies report raw weight not BMI. On the other hand, this study included only healthy women, so the findings observed may be a good representation of healthy plasma volume expansion for comparisons (e.g., if data on plasma volume in women with obesity are collected).
Body position is important for measurements and there were several different positions (e.g., lying on side, sitting reclined) employed in the studies, or it was not clearly reported. Future work should standardize the position during the measurement. There is also a strong interest in the range of normal plasma volume, not just the mean, but this was only reported for the peak plasma volume expansion in one study [14].
A strength and unique aspect of this review was that we included only longitudinal studies, which had as many as eight repeated measurements during pregnancy and which always measured nonpregnant plasma volume in the same cohort of women. As well, 17 separate gestational time points in pregnancy were represented and plasma volume was always measured by “direct” methods, rather than indirect methods such as calculations based on hemoglobin and hematocrit changes. We assessed numerous aspects of the available data, including the maximum change, the change up to discrete gestational intervals, the rate of change between gestational intervals, and important aspects from individual studies.
{kind=link}
{kind=link}