In this prospective observational study, we aimed to investigate the efficacy and safety of different OPT course in adult NMDAR encephalitis. Our study is the first of its kind, providing valuable insights into the optimal treatment duration for this condition. Here, we summarize our main findings: (1) The proportion of responders at 3 months after initial treatment was significantly higher in Group ≤ 3 mo and Group 3–6 mo compared to Group > 6 mo. However, after propensity score matching, no significant improvement in outcomes, including the proportion of responders and the degree of mRS change at different time points, was evident for OPT courses lasting more than 3 months. (2) Over a 2-year follow-up, the three groups showed no significant differences in relapse risk, the proportion of patients who fully recovered from onset, time to total recovery, residual symptom impact on daily life or CASE scores. (3) Group > 6 mo received higher prednisone doses and experienced more adverse events, particularly weight gain. Overall, our study suggests that extending the oral prednisone course beyond 3 months in adult NMDAR encephalitis may not lead to further improvements in clinical outcomes. Moreover, it increases the risk of adverse events, primarily weight gain. These findings contribute to the understanding of treatment strategies for NMDAR encephalitis and have practical implications for optimizing patient care.
The common OPT strategy is to initiate oral prednisone at 1–2 mg/kg/day, often followed by a gradual taper over several weeks to months [25]. However, the optimal treatment duration is uncertain. Our study suggests that extending oral prednisone beyond 3 months may not yield notable improvements in neurological function. We observed no benefits in the number of respondents, changes in mRS scores, mRS scores at various time points, CASE scores, changes in CASE scores, favorable outcomes (mRS ≤ 2), total recovery rate within 2 years, or residual symptom impact on daily life for oral prednisone for over three months. Our findings align with a retrospective pediatric study of 190 children with NMDAR encephalitis, which found no significant differences in recovery rates between long-term and short-term oral prednisone treatments [26]. In a recent report by Li et al., which focused on autoimmune encephalitis, the choice of OPT course, in combination with MMF, did not significantly affect patient outcomes [21]. However, it's worth noting that this study had a small cohort and didn't investigate the benefits of a shorter taper within the initial 3 months.
Intravenous methylprednisolone is the guideline-recommended first-line treatment for NMDAR encephalitis [27]. Prednisone tapering regimens vary considerably in clinical practice. Decisions about treatment duration should consider the patient's clinical status, treatment response, tolerance, and safety. Our study shows that neurologists tend to prescribe oral prednisone for over 6 months, especially for patients with consciousness disorders and high CSF antibody titers. Additionally, previous research has indicated that physicians may extend oral prednisone courses based on the presence of MRI abnormalities [21]. Although these factors may be linked to a worse prognosis [28–31], our propensity score-matched analysis didn't find significant differences among the OPT groups. This suggests that clinical decisions to prolong prednisone treatment based solely on these factors may not always be justified, emphasizing the need for evidence-based guidance.
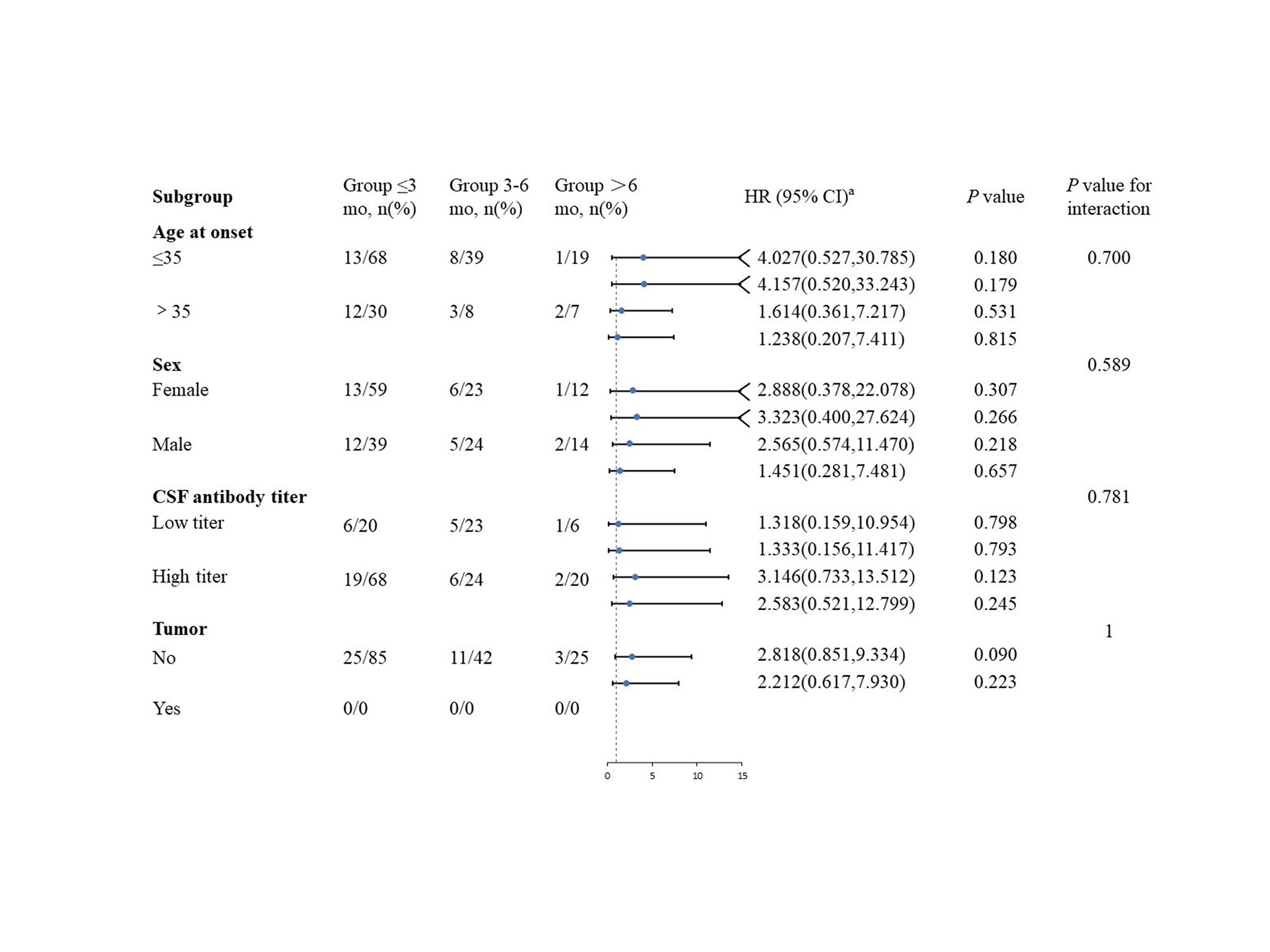
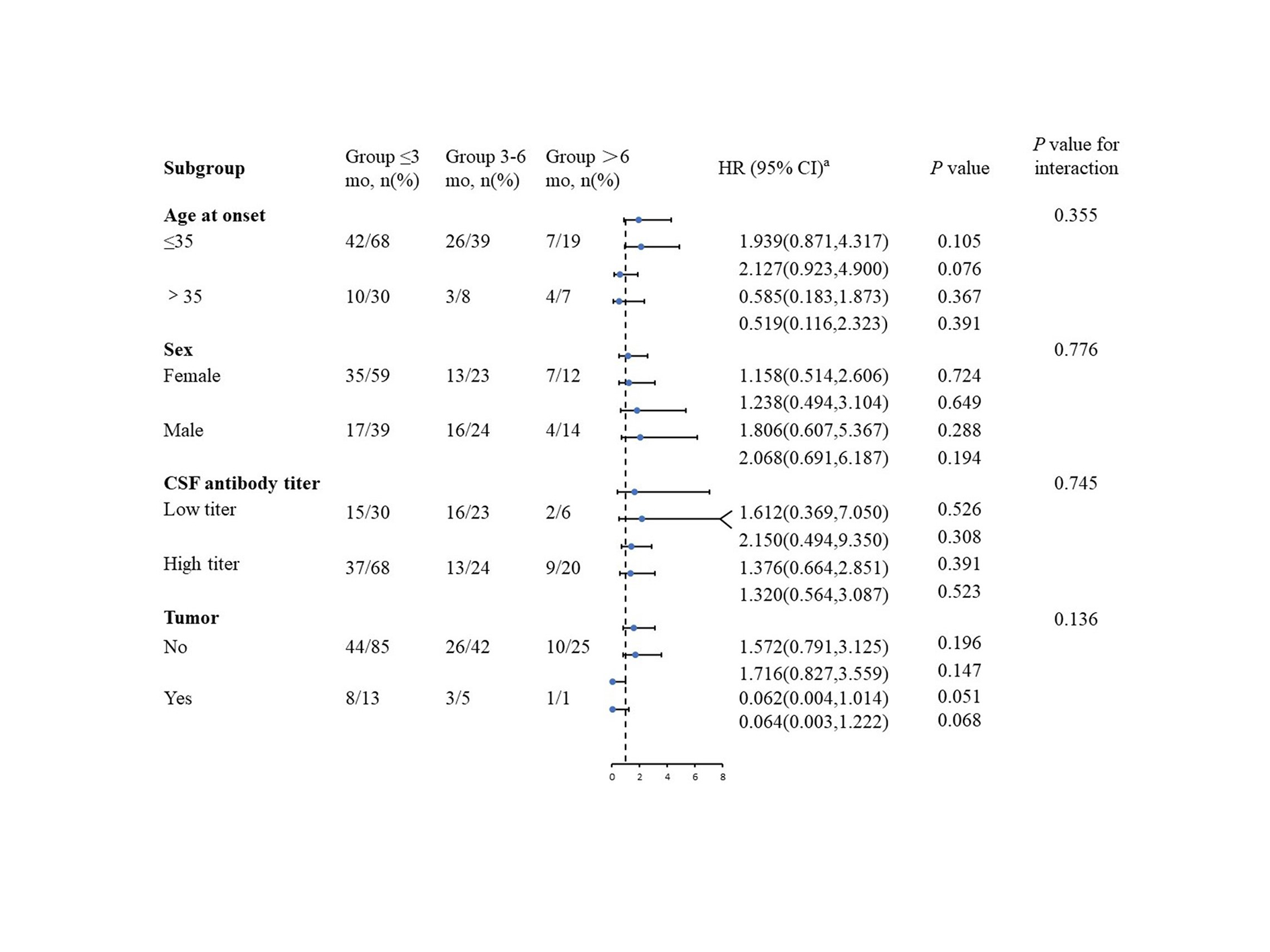
Our study observed variations in treatment responses among male patients, patients without tumors, and patients with high CSF antibody titers. Patients in Group ≤ 3 months showed better short-term responses (more responders at 3 months after initial treatment) and better long-term prognosis (CASE scores at 12 months). Prior research has identified risk factors for outcomes in NMDAR encephalitis, including ovarian teratoma, male gender, and high CSF antibody titers [30, 32, 33]. While patients without ovarian teratoma who received ≤ 3 months of OPT had expectedly better short-term prognosis, it's intriguing that male patients or those with high CSF antibody titers also showed improved short-term outcomes. However, the limited sample size and the absence of propensity matching in our subgroup analysis may introduce baseline confounding factors.
Experts recommend avoiding shorter steroid tapering in autoimmune encephalitis cases with poor initial responses [34]. However, these recommendations lack robust supporting evidence. Our data shows that 49.1% of individuals experienced symptom improvement at 1 month after treatment, with no significant differences in long-term outcomes between patients with good or poor initial responses across the three OPT courses. Notably, due to the limited sample size within each subgroup, propensity score matching was not feasible. Thus, further investigations are warranted to validate these preliminary observations.
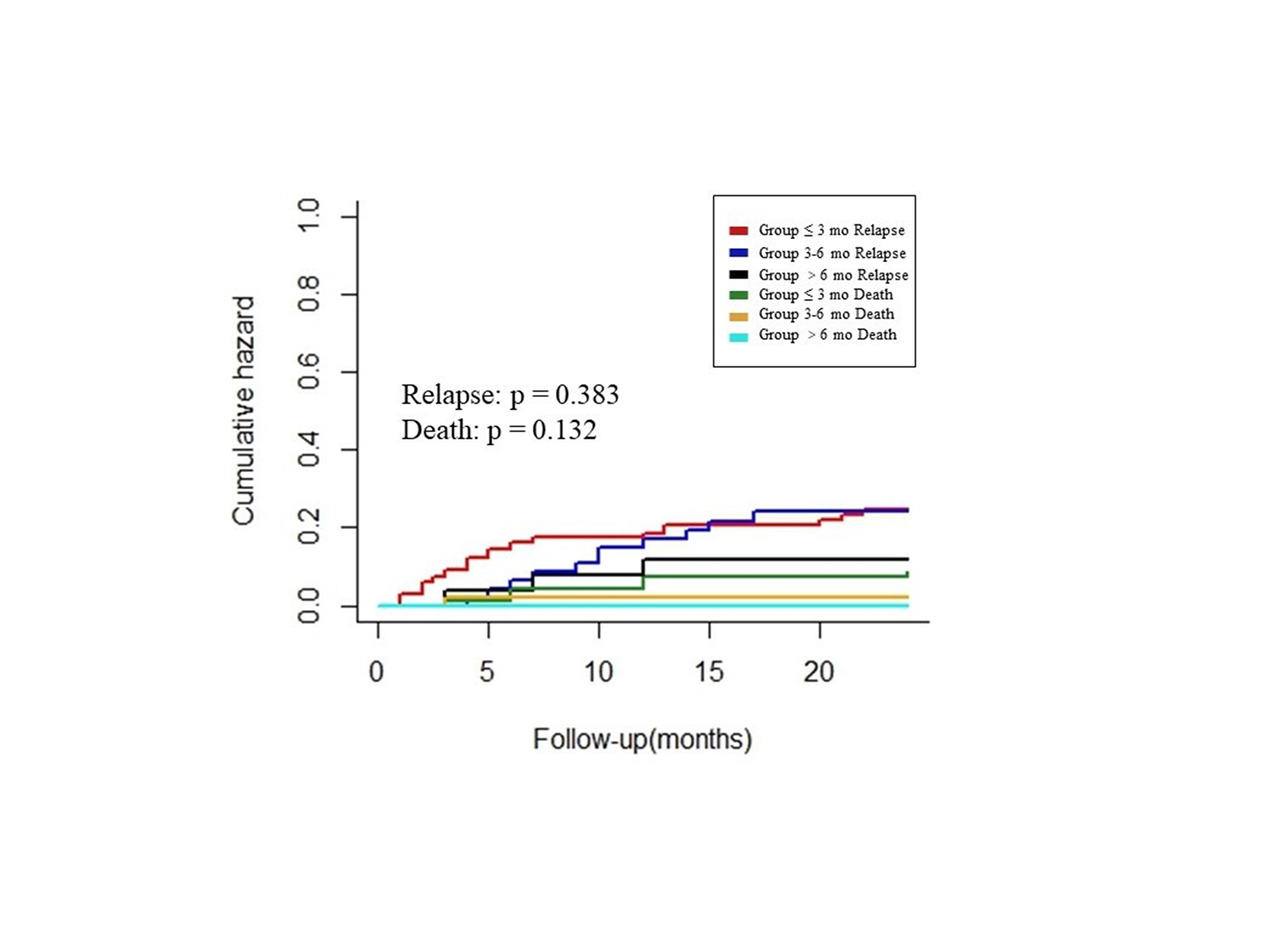
Our study found no significant differences in the risk of relapse within a 2-year period among the three OPT groups, regardless of age, sex, CSF antibody titers, or tumor presence. These results emphasize that oral prednisone alone may not be the primary strategy for preventing relapses in NMDAR encephalitis. In our study, 22.8% of participants experiencing relapses within 2 years. Notably, 9.4% of patients relapsed during the course of oral prednisone, suggesting that the risk of relapse persists despite such treatment. The literature on the efficacy of oral prednisone course in preventing relapse is limited. As far as we know, only one retrospective pediatric cohort study has explored the relationship between OPT courses and relapse rates in NMDAR encephalitis [26]. Previous research indicated that corticosteroids exhibit limited specificity in countering antibody-mediated immune responses, rendering them insufficient to mitigate the autoantibody-mediated immune processes [35, 36]. Importantly, combining corticosteroids with second-line immunosuppressive agents may hold promise for reducing relapses [37–39].
Corticosteroids are commonly employed in the treatment of various autoimmune diseases due to their anti-inflammatory and immunosuppressive properties. The optimal duration of corticosteroid tapering, however, varies across different diseases, possibly due to distinct disease mechanisms and corticosteroid involvement in signaling pathways. For example, in MG, an autoimmune disease with antibodies targeting neuromuscular junction proteins, long-term, low-dose corticosteroids are recommended to suppress immune responses [40]. Corticosteroids reduce germinal centers and modulate chemokines and angiogenesis, possibly through acetylation [41]. This is in contrast to CIDP, where long-term corticosteroid use is associated with reductions in the frequencies of total CD4 + T cells, CD4 + memory subsets, and natural killer (NK) cells, contributing to its efficacy [42]. In NMDAR encephalitis, the mechanisms underlying long-term corticosteroid response remain unclear, with a possible interaction between the NMDA receptor system and the glucocorticoid pathway influencing neuronal signaling [43]. Further research is needed to elucidate these mechanisms and guide the development of more targeted and effective treatment regimens.
Long-term corticosteroid use is associated with adverse events [4, 5, 11, 44]. Patients receiving oral prednisone for over 3 months are more likely to experience weight gain and higher cumulative prednisone doses. Reducing the cumulative dose is crucial as complications increase with dose [45]. Another study has similarly reported an increased risk of weight gain in autoimmune encephalitis patients receiving long-term oral prednisone [21]. Notably, obesity can lead to various comorbidities such as hypertension and cardiovascular events [46]. In addition, corticosteroids may induce or exacerbate psychiatric symptoms in NMDAR encephalitis, such as depression, insomnia, agitation, and psychosis [35]. However, our study did not find similar symptoms. In summary, oral prednisone for ≤ 3 months offers a safer alternative when comparable efficacy to longer courses is observed, favoring a shorter OPT course.
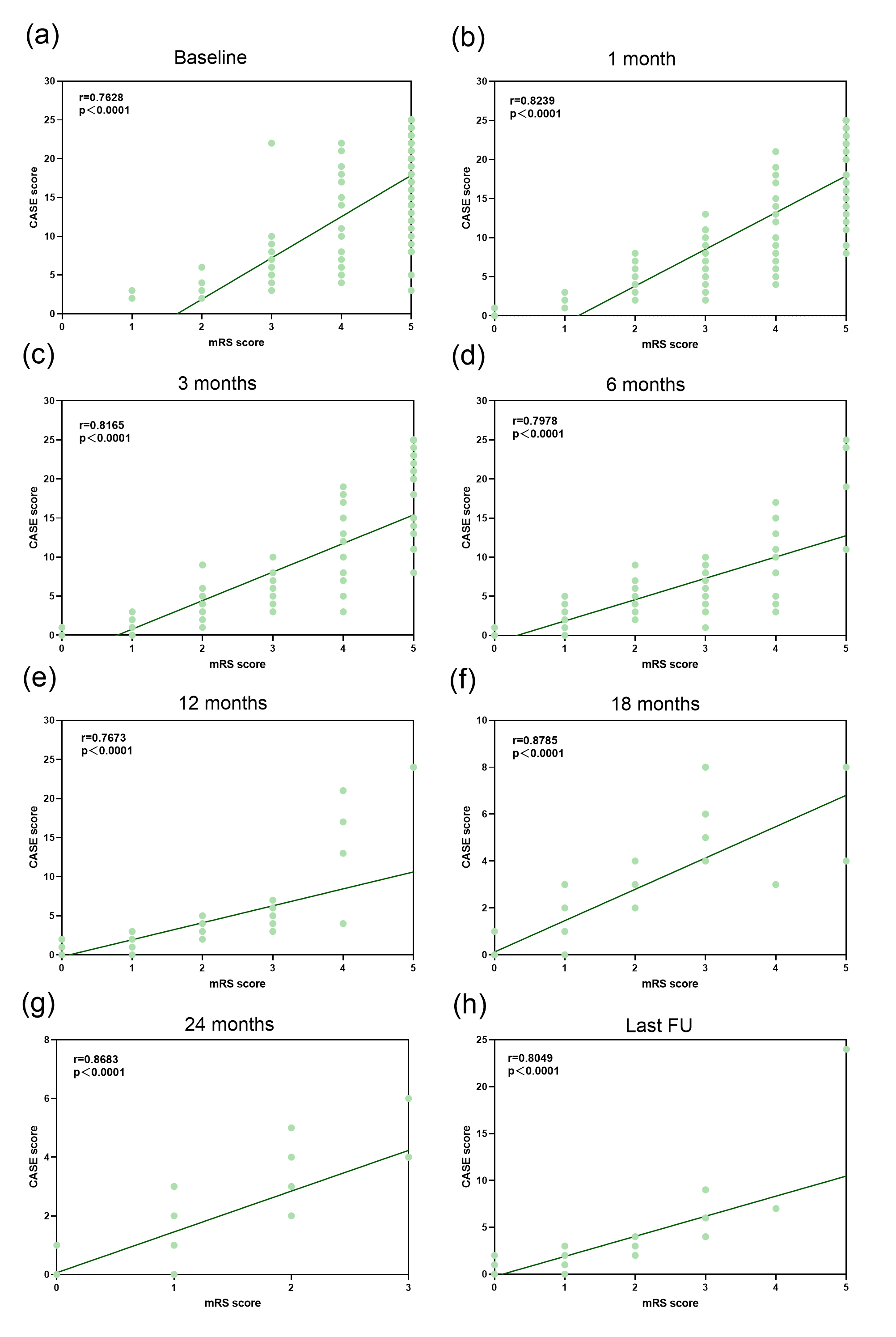
However, this study has several limitations. Although we applied the propensity score matching to balance baseline covariates and our study findings were consistent with insensitivity analyses, potential bias caused by unmeasured and unobserved factors cannot be completely ruled out. RCTs with standardized OPT protocols are vital to evaluate benefits and risk. Furthermore, the generalizability of our findings is restricted by the study's exclusive enrollment of Asian participants and the uniform use of prednisone, which may not apply to individuals from diverse racial backgrounds or those treated with different corticosteroids. Additionally, diverse antibody subtypes in autoimmune encephalitis may result in distinct treatment responses, necessitating further research stratified by antibody subtype. Moreover, the impact of symptomatic medications on mRS scores should also be considered. In addition, our prior study and a meta-analysis have established that combination therapy during the acute phase is more effective than monotherapy [14, 27]. Consequently, most patients in this study received combination therapy. Even though we used propensity score matching and excluded patients who received IVIG and PE within one month before prednisone treatment, the potential synergistic effects of PE and IVIG cannot be ruled out entirely. Finally, although we used CASE scores to assess the severity of disability, that lacks evaluations of sleep and neuropsychological assessments such as Pittsburgh Sleep Quality Index, Hamilton Depression Scale (HAMD) and Hamilton Anxiety Scale (HAMA).
{kind=link}
{kind=link}
{kind=link}
{kind=link}