This study is the first, to our knowledge, to examine the differences in PO and ADL based on SB time among older CVD patients. While several previous studies have investigated the impact of SB time and/or physical activity in hospitalized patients [9, 15, 16], this research specifically focused on older CVD patients. We investigated the cut-off values of SB time based on methods used in previous studies [28, 32]. In a recent study in Japan, Kono et al. reported that non-lying time could be one of the associated factors of HAFD in older patients undergoing TAVI [17]. They suggested that non-lying time of about 480 min (8 h) during hospitalization may be an initial target for preventing HAFD. Therefore, on the basis of these previous studies, we considered the cut-off value used for SB time to be appropriate.
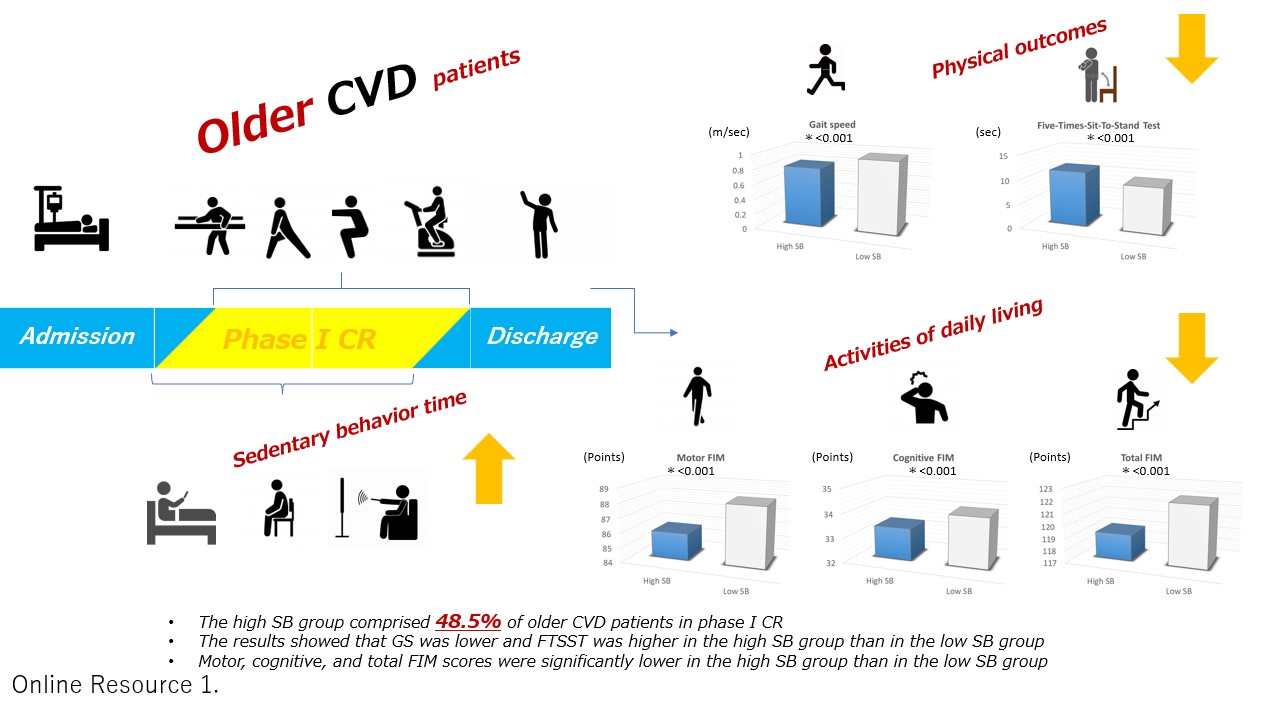
Cattanach et al. previously reported that patients were observed to be in bed 51% of the time, sitting out of bed 43% of the time, standing 1% of the time, and walking 5% of the time. In addition, the response to a questionnaire they used indicated that one third of the participants were not observed to walk during the observation period. Moreover, 38% of the participants had expected to remain in bed while in hospital [15]. Even though the assessment methods between their study and ours were different, the present study showed a high rate of SB of 48.5%. In our previous study [28], which included both middle-aged and older patients, a high rate of SB of 47.6% was shown. However, the rate of SB was higher in the present study as it was limited only to older patients. In other previous studies, while there are differences in diseases and ages of the study patients, they also showed that older patients tend to engage in more sitting SB time and spend more time in bed [13, 14]. In their systematic review, Harvey et al. [36] suggested that older adults (age ≥ 60 years) are one of the most sedentary groups in society, spending on average 80% of their time in a seated posture with 67% being sedentary for more than 8.5 hours per day. In the present study, the total sitting SB time in the high SB group was 718.42 min/day, which converts to approximately 11.97 h/day. Because SB occurred primarily during leisure time, outside of phase I CR, the greatest reduction in total SB time can likely be achieved by targeting leisure time sedentary activities during hospitalization, with particular attention paid to older CVD patients with high SB. We consider it important to address this problem beginning in phase I CR because as reported by Chastain et al. [37], the effectiveness of interventions to reduce SB in community-dwelling older adults remains unclear.
There were significant differences in the characteristics of age, employment, and main diagnosis between the patients in the two study groups. Notably, these factors largely align with predictors of high SB levels in the general population and of several diseases [9, 20, 26, 27, 38, 39]. Our findings suggest that these factors may also impact high SB levels in older CVD patients.
With regard to PO, GS was lower and the FTSST was higher (Table 2, Fig. 2) in the high SB group than in the low SB group after adjusting for baseline characteristics. Individuals whose GS is below 1.0 m/sec are at high risk for leg injury, hospitalization, and death [22, 40]. In terms of traffic signal programming for pedestrians in Japan, a GS of 1.0 m/sec or faster is required to cross the street within the programmed period [22]. Thus, a GS of 1.0 m/sec or faster is an important ability that is needed for various public activities such as shopping, hobbies, and work after discharge from hospital. The value was close to 1.0 m/sec for the low SB group, but for the high SB group, it was much lower than 1.0 m/sec.
The FTSST value in the high SB group was 11.31 sec, similar to the low physical performance value of the AWGS 2019 (≥ 12 sec) [23]. In addition, Camarzana et al. recently suggested that the FTSST was an independent predictor of 1-year mortality in patients with severe aortic stenosis who did not undergo valve replacement (59 patients; age, 86.1 years) [41]. Therefore, the reserve capacity for GS in the high SB group is low, and FTSST time is high, indicating that special attention should be paid to older CVD patients.
Motor, cognitive, and total FIM scores were significantly lower in the high SB group compared to the low SB group (Table 2, Figs. 3 and 4). A previous study aimed to identify predictive factors for ADL as assessed by FIM at discharge in older heart failure patients with preserved ejection fraction. The receiver operating characteristic curves yielded cutoff values for predicting ADL at discharge of 34.5 points for the motor FIM score and 28.5 points for the cognitive FIM score. Notably, the motor and cognitive FIM scores in the high SB group of the present study included patients with scores ‘above’ these reported thresholds, potentially minimizing the impact of SB on discharge results. However, other previous studies have suggested that FIM scores at discharge serve as independent predictors of re-admission and mortality at 90 and 180 days in CVD patients [25, 42]. Kitamura et al. further classified older heart failure patients into four groups based on a previous study’s cutoff values for the Geriatric Nutritional Risk Index (GNRI), an index of nutrition, and motor-FIM. They reported that the rate of readmission avoidance was significantly lower in the group with GNRI < 92 and motor FIM < 75 within 90 days of discharge [25].
Iwata et al. also investigated the prognostic impact of the FIM score on clinical outcomes in hospitalized patients with acute decompensated heart failure (ADHF). They retrospectively analysed 473 ADHF patients with available pre-discharge FIM scores admitted to their institution. The primary outcome measures, defined as a composite of 180-day all-cause deaths and readmissions, were compared among three tertiles [42]. The median total FIM score was 102 (interquartile range: 85–115). Tertile 1 corresponded to an FIM score > 111, Tertile 2 to that of 90–111, and Tertile 3 to that of < 90. Even after multivariable adjustment, the results remained significant [Tertile 1 vs. 3: adjusted hazard ratio, 3.28; Tertile 2 vs. 3: 2.32]. FIM scores were significantly associated with readmission or death within 180 days of discharge in hospitalized ADHF patients [42].
Consideration of the FIM scores at the time of discharge, especially in relation to high SB, is crucial. Additionally, prognosis after discharge must be taken into account and measures implemented with a view to continuing phase II CR. Although our study focused on phase I CR in older CVD patients, it is worth noting that in a different context (long-term acute care hospitals for patients after stroke), changes in FIM scores associated with the minimal clinically important difference were 22 points for total FIM, 17 points for motor FIM, and 3 points for cognitive FIM scores [43]. Although we did not specifically examine improvement in pre- versus post-FIM scores during phase I CR, ADL of the high SB group were significantly lower at discharge. Thus, older CVD patients with high SB are likely to experience not only loss of motor function but also a decline in cognitive function related to ADL in the future. It may be necessary for staff in charge of phase I CR to intervene for patients with SB during hospitalization to improve their ADL.
Our study showed that high age, heart failure, and unemployment tended to be associated with high SB. As mentioned earlier, even though hospitalized patients with acute heart failure infrequently experience hospital-associated disability, only 44% of these patients were accepted into phase I CR [8]. Therefore, greater attention should be paid to these factors during phase I CR. Early mobilization to reduce SB, early screening for sarcopenia, and implementing aerobic exercise and resistance training during hospitalization are essential components of phase I CR.
Limitations
Several limitations need to be considered in the present study. First, the study is constrained by its small sample size and the limited number of female patients, which hindered the assessment of sex-related differences. Second, many of the older CVD patients were hospitalized solely for therapeutic interventions, such as pacemaker battery replacement, and were therefore excluded from this study, which may have introduced selection bias. Third, the study included various CVDs as the primary diagnosis, along with comorbidities requiring different treatments. Fourth, a self-reported subjective questionnaire was used to assess SB time, and the study lacked objective measurements made by a versatile device with various features and tools. Finally, we were unable to investigate the relationship between SB time and prognosis, including re-admission rates and mortality. Notably, SB has been linked to acute detrimental effects on vascular function, blood pressure, and lipid levels, which may contribute to the risk of cardiovascular events and mortality [26, 27, 44].
The recent systematic review by Chastin et al. suggested that it remains unclear whether interventions to reduce SB are effective in decreasing sedentary time in community-dwelling older adults [37]. Furthermore, the impact of these interventions on the physical and mental health of community-dwelling older adults remains uncertain. Thus, further research is necessary to explore interventions aimed at reducing high SB and improving both PO and ADL of older CVD patients during phase I CR.
{kind=link}