Ethical Considerations
This present study was conducted in accordance with the 2020 ARRIVE Guidelines (17). The protocol of this study was approved by the vice chancellor for research of the Mashhad University of Medical Sciences (no. 971876) and the Organizational/Regional Ethics Committee of Mashhad University of Medical Sciences on April 5, 2019 (Approval Code: IR.MUMS.DENTISTRY.REC.1398.065).
Preparation of dogs
Selected for the current research were eight 4-month-old male mongrel dogs with intact dentition, healthy periodontium, and a body weight of around 10 ± 2 kilograms. In order to better adapt to their new environment and diet, the animals were housed separately in individual cages for a period of 15 days prior to the operation. During this time, vaccination and deworming treatments were carried out. All the dogs received polyvalent and rabies vaccines (Biocan, Zchesh) as well as antiparasitic treatment (Ivermectin SC, Alfasan and Topkim tablets, Droncomplex). Following the exfoliation of the dogs’ primary teeth, biweekly radiographs were taken of the incisor teeth in a parallel manner to check their readiness to enter the study. (Figure 1)
Figure 1. Initial radiographs of the upper (A) and lower (B) incisor teeth at the beginning of the study
The groups and Sample Size Calculation
The teeth in the present study were placed in one of these 5 groups: 1- Negative control group, 2- Positive control group, 3- i-PRF group, 4- i-PRF+ PDLSCs group, 5- GTR group. (Figure 2)
Considering a confidence level of 0.95 and 80% power and using the values for the mean and standard deviation from a previous study )comparing PDLSCs and control groups)(6), the sample size was 4.34. To ensure higher certainty, the current study included six teeth in each (n=6) group and according to the five study groups, 30 teeth were considered for the current study.
Samples & Randomization
The present research utilized five teeth from each dog (two maxillary anterior teeth and three mandibular anterior teeth). According to the sample size of 30, six dogs were needed. However, having taken into account the probability of a series of sample drop-outs during the surgical procedure (such as closed apices or root fractures during the tooth extraction), the current study deemed the required number of dogs to be eight. First, the numbers 1 to 8 were randomly assigned to the dogs. Then, the desired teeth were coded, starting with number 1 (upper right second anterior tooth) in dog No. 1 up to number 30 (lower left third anterior tooth) in dog No. 6. After that, with the usage of the Research Randomizer site (http://Randomizer.org), six sets of five unique numbers were generated to determine which group each tooth belongs to. If a sample was excluded from the study during surgery, it was randomly replaced with one of the ten teeth from the remaining two dogs (dogs No. 7 and 8).
Preparation of PDL Stem Cells Bank
The present research extracted PDLSCs by employing the collagenase and dispase method. Human premature premolar teeth, extracted for orthodontic purposes, were transferred to a culture medium. To uphold infection control principles, the desired tooth crown was rinsed with chlorhexidine before extraction. Each tooth was placed in a sterile Falcon tube containing 10 milliliters of alpha-MEM culture medium (Modified Eagle Medium) from Sigma-Aldrich/USA, 1% penicillin/streptomycin antibiotic, and 5 micrograms per milliliter of amphotericin. The tubes were then quickly transferred to the Immunogenetics Department of the Bu Ali Research Center. Each tooth was moved under completely sterile conditions to a Class 2 laminar hood. Then, the middle third of the root surface was trimmed with a sterile scalpel blade and collected (in a thin layer) in a sterile petri dish containing a small amount of culture medium. The trimmed contents were transferred to a T-25cm² culture flask (SPL Life Sciences, Korea) with a sampler tip. A small amount (1 to 2 milliliters) of complete alpha-MEM culture medium (containing 20% Fetal Bovine Serum (FBS) and 1% penicillin/streptomycin antibiotic (100 micrograms per milliliter)) (Gibco/USA) was added to the flask. All the flasks were then transferred to CO2 incubator and were to remain there for about 2 to 3 weeks without undergoing any severe shaking. Additionally, a small amount of complete culture medium (approximately 500 microliters) could be added to each flask weekly. After approximately 10 days, microscopic examination of the flasks began. If colonies of spindle-shaped cells were observed, each flask could then be washed twice with a sterile Phosphate-buffered saline (PBS) (Gibco, USA) solution to remove excess contents, leaving only the spindle-shaped cells adhering to the flask bottom. Next, 5 ML of complete culture medium were added to each flask, which was then placed in an incubator at 37 degrees Celsius (with 5% CO2). Every 3 to 4 days, the cell culture medium was replaced once with a fresh complete medium. Once the flask bottom was filled with spindle-shaped cells and reaches 80-90% confluency, the cells were passaged. This was accomplished by adding about 2-3 milliliters of trypsin enzyme (Trypsin EDTA, Cegrogen, Germany) to each flask and transferring the flasks to the incubator, leaving them for 2-5 minutes for the trypsin enzyme to take effect. Afterwards, gentle taps were applied to the corners of the flask. The cells were observed under an inverted microscope (Olympus, Japan) until they became round, single, separated, and floating. It was necessary to avoid prolonged exposure of cells to trypsin as it can be toxic and lead to cell degradation. After ensuring cell detachment, the trypsin was neutralized and the cell-containing medium was transferred to a Falcon tube for centrifugation. The resulting cellular pellet was resuspended, divided into larger flasks, and supplemented with culture medium. The cells attached and proliferated, progressing through passages until reaching the third passage (P3) for further characterization:
1. Microscopic Examination: The cells extracted from PDL exhibited fibroblast-like, elongated shapes and adhered to the surface of flasks and plastic containers. They could be observed under an inverted light microscope after seven days. (Figure 3)
Figure 3. Inverted microscope image of undifferentiated human PDL stem cells after seven days (× 400)
2. Flow Cytometry Assay: The process started by emptying a T175 flask that had reached 90% confluence, followed by trypsinization and resuspension in PBS with 5% FBS. Then, antibodies, such as CD90, CD73, and CD105, were added. Flow cytometry results indicated that the mesenchymal stem cells were negative for the CD34 and CD45 markers and positive for the CD90 marker. (Figure 4)
Figure 4. Immunophenotypic identification of mesenchymal stem cells derived from the PDL of human teeth by flow cytometry for the expression of mesenchymal stem cells (CD90) and hematopoietic (CD34, CD45) markers.
3. Differentiation Tests:
A. Differentiation to Bone: The stem cells were transferred to two six-well plates and cultured until confluence. An osteogenic differentiation medium was added and replaced twice a week for 3 weeks. Afterward, Alizarin red stain was utilized to detect calcium ions in the extracellular matrix. The formation of a mineralized matrix was indicated by a reddish-orange color.
B. Differentiation to Adipocytes: Similar to the bone differentiation test, the stem cells were transferred to six-well plates. An adipogenic differentiation medium was added to the wells and replaced twice a week for 3 weeks. At the end of this period, Oil Red stain was added to identify lipid droplets, indicating differentiation into adipocytes.
Preparing the Amniotic Membrane Scaffold
After the cells reached the necessary confluency in the P3 and underwent the characterization process, they were prepared for transfer onto the amniotic membrane. This natural scaffold is a type of acellular amniotic membrane designed for performing biological procedures.
Multiple studies have shown that lyophilization preserves the histological tissue structure of the human amniotic membrane (18). The present study employed lyophilized amniotic membranes (SinaCell, Tehran, Iran).
After the trypsinization of cells from the flask and the creation of a cellular suspension, the cells were counted under a Neubauer chamber, and one million cells were homogenized in one milliliter (106 cell/milliliter). The amniotic membrane was placed in a sterile Petri dish containing a small amount of PBS (one milliliter) under sterile conditions. The membrane was uncovered with sterile tweezers, and the side of the membrane, where the cells would be placed, was gently lifted and removed from the dish. This process involved washing the membrane with a small amount of PBS buffer to maintain moisture. The PBS buffer was then removed from the Petri dish, and the edges of the membrane were opened and flattened by the usage of sterile tweezers. Multiple transfers of cells onto the membrane were performed using a sampler, with approximately 20 microliters of cell suspension added each time. The Petri dish was left uncovered for the cells to penetrate the membrane, a process known as seeding. Between each seeding session, a waiting period of 30-40 minutes allowed the cells to adhere to the scaffold, while regular checks prevented the membrane from drying out. If dryness was observed, additional cell suspension was added until all the cells were employed. Finally, a small amount of alpha-MEM cell culture medium was applied to the membrane and its edges in order to prevent drying and provide nutrients. The Petri dish was then sealed and transferred to a CO2 incubator containing 5% CO2 at a temperature of 37 degrees Celsius under sterile conditions. Twenty-four hours were allowed for the cells to adhere to the membrane. During this time, it was vital not to disturb or shake the Petri dish to prevent the membrane from shifting. After 24 hours, the membrane was ready to be transferred for dental replantation. On the day of surgery, the prepared membranes, in separate Petri dishes, were transported in a cold box to the Animal Research Center of the Dental School of Mashhad University of Medical Sciences. Figure 5 is a view of the Scanning Electron Microscope (SEM) image showing the attachment of undifferentiated human PDL stem cells to the amniotic membrane.
Figure 5. Scanning Electron Microscope (SEM) image shows undifferentiated human PDL stem cells attached to the amniotic membrane.
To prepare the stem cells for injection, the same third-passage cells were dissolved in a volume of 500,000 cells in 0.2 milliliters of PBS buffer. They were then drawn into a syringe and prepared for injection into the alveolar socket of the fourth group.
i-PRF Preparation
Ten milliliters of blood were drawn from the animal's vein and quickly transferred to specialized tubes for PRF preparation. The tubes were then placed inside a centrifuge machine (Universal (D.G.T 8), Iran). In accordance with the manufacturer's recommendation, the centrifuge machine was set to a speed of 3000 rpm and a time of one minute for i-PRF preparation. Subsequently, using an 18-gauge needle, the upper portion of the tube contents was extracted and employed for further procedures. (Figure 6/A) It is worth mentioning that, in a pilot study conducted on four dogs, the cellular content of i-PRF, prepared according to this method, was examined and validated.
Figure 6. (A) The prepared i-PRF (B) The teeth soaked in i-PRF (C) The tooth after being removed from the i-PRF.
The Surgical Procedure
Given the variability in dental maturation timing, the present study made every effort to schedule the surgical procedures in such a way that the apical sizes of the developing teeth would be similar during surgery. Based on the established schedule for each dog's surgery (determined through serial PA radiographs obtained in parallel), the days for operating on the lower jaw and upper jaw were identified. It was not mandatory to perform surgery on both jaws at the same time.
1. Anesthesia Protocol
In preparation for surgery, the dogs were fasted for 12 hours, but still had access to water. On the surgery day, for all the animal experiments, the current research performed the induction phase of general anesthesia with acepromazine maleate (Alfasan; 0.01 milligrams/kilogram; IM) and ketamine-diazepam (Alfasan, 10 mg/kilogram and 0.2 ml/kg; IV). This anesthesia was maintained during the surgical procedure at a constant rate infusion (CRI) of a 10% ketamine chloride solution in Ringer's solution. Throughout all stages of anesthesia, the vital signs of the dogs, including heart rate, body temperature, respiratory rate, and depth of anesthesia, were carefully monitored.
2. Tooth Extraction
For tooth extraction, the animal's head was positioned in a specific manner. Then, prior to tooth extraction, local anesthesia was administered by injecting a combination of 2% lidocaine and 1:100,000 epinephrine.
All tooth extractions were performed by a single dentist. The teeth were extracted with as little trauma as possible and by utilizing specially adapted forceps for dogs.
First, the root surface was washed with normal sterile saline. Then, the teeth were placed coronally on pre-embedded wax points on the summary sheet and left in a dry environment for 70 minutes (delayed replantation)- except for the first group whose time was 10 minutes (immediate replantation).
3. Tooth preparation protocol and replantation
The therapeutic stages of each of the five treatment groups following tooth extraction consisted of various methods of tooth preparation and replantation:
Group 1: The Negative Control Group involved immediate placement (after a 10-minute break in a dry environment) of the tooth after a saline wash and temporary splinting. Group 2: The Positive Control Group employed delayed placement after a saline wash. Group 3: The i-PRF Group featured a delayed placement of the tooth after it had been soaked in i-PRF for 5 minutes. (Figure 6/B & C) Group 4: The i-PRF+ PDLSCs Group involved the application of i-PRF on the tooth root (similar to the group 3) and, followed by injection of the PDLSCs into the alveolar socket (500000 cells/0.2 ml). Group 5: The GTR Group also applied i-PRF and PDLSCs on the tooth root, but introduced an amniotic membrane. This process called for applying i-PRF to the PDLSCs-seeded amniotic membrane, and carefully wrapping the membrane around the tooth root before replanting and splinting the tooth.
Before the replantation of each tooth, the corresponding alveolar socket was thoroughly washed with 20 milliliters of normal saline to remove any formed clots.
After the replantation, all teeth in one jaw were splinted using a 0.6 orthodontic wire and flowable composite. The splint extended to a healthy tooth on each side. Excess wire was removed, the occlusion checked, and interferences addressed.
Post-surgery procedures involved pain control with Meloxicam (0.2 milligrams/kilogram SC for three days), and infection prevention with Cefazolin vial 1 gr (22 milligrams/kilogram IV before surgery and an hour after surgery) and Penicillin vial 6.3.3 (at a dosage of 50000 units/kilogram IM once per day for three days following surgery). The dogs were provided with a soft diet for a duration of 8 weeks to minimize the risk of mechanical disturbances. Splinting lasted for 10 days for all dental groups except for the GTR Group, which required an additional week.
Evaluation
Clinical assessments were made at the one-month and two-month follow-ups for all the groups. The check-ups focused on changes in tooth color, mobility, percussion sound, and possible presence of fistula or abscess. These factors were examined to identify potential pulp necrosis or pathological mobility (Grade 2 and 3 on the Miller scale (19)). At specific time intervals, radiographic evaluations were also conducted post-anesthesia, with the use of parallel technique PA radiography. Radiographs were standardized by employing aluminum foil markers. Specific radiographic criteria, such as periapical radiolucency, external root inflammation, root replacement, and internal root resorption, were assessed independently by two blind dentists.
Ultimately, at the end of the second month, the animals were sedated and euthanized post-surgery with an intravenous overdose of pentobarbital sodium 3% at a dosage of 30 mg/kg (supplied by Shimi Darou Parsian Co, Tehran, Iran). Following euthanasia, each dog underwent perfusion with a 4% formaldehyde solution (obtained from Merck, Darmstadt, Germany) via the carotid artery. Block sections of anterior portion of the maxilla and mandible were dissected, fixed in 10% buffered formalin, decalcified in a 15% solution of ethylenediaminetetraacetic acid (EDTA, Hongyan, Tianjin, China) at pH 6.8, trimmed and dehydrated. The blocks were embedded in paraffin and sectioned perpendicular to the long axis of the teeth at a thickness of 5 µm and at 500 µm intervals in the apical and middle third of the roots. At each sectioning level, sections were stained with hematoxylin-eosin (HE). (20-22)
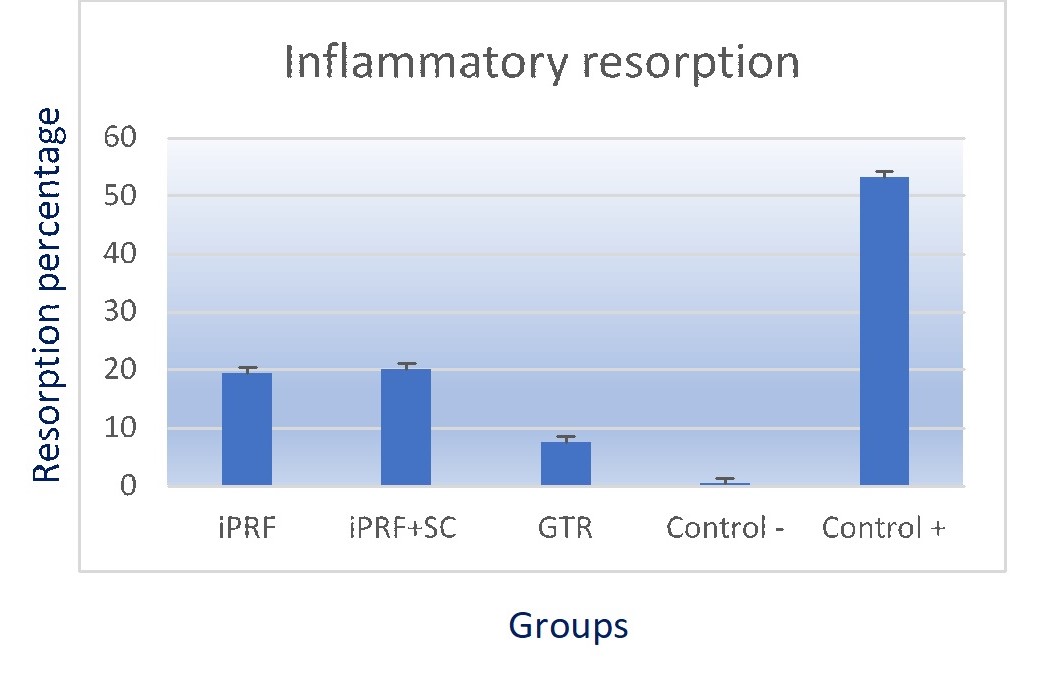
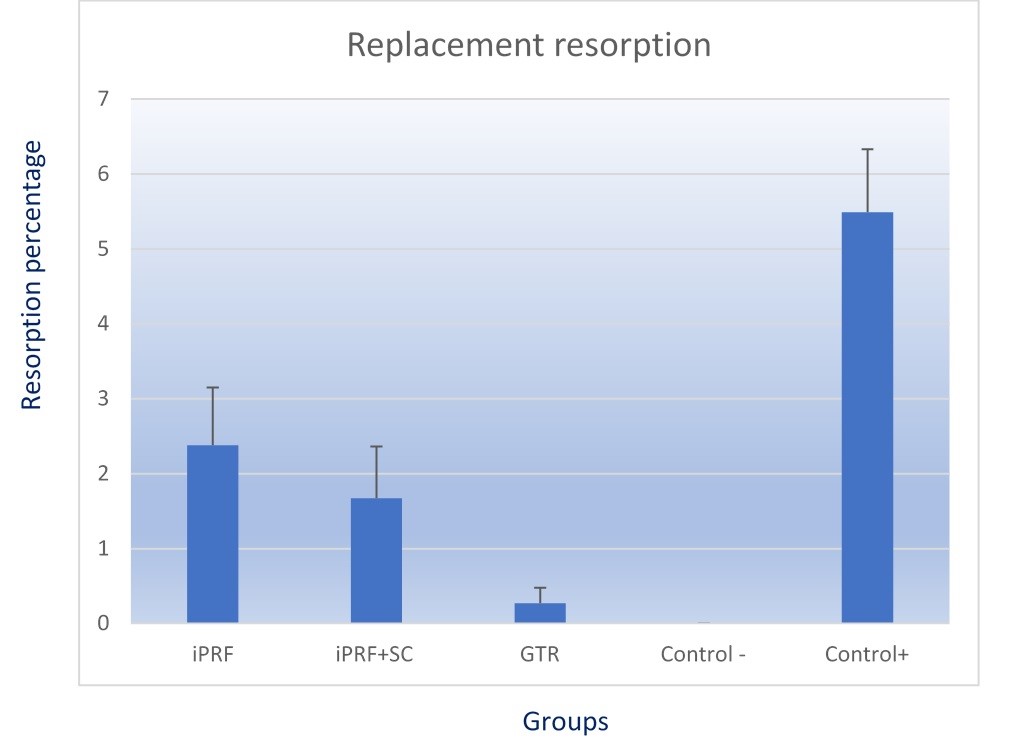
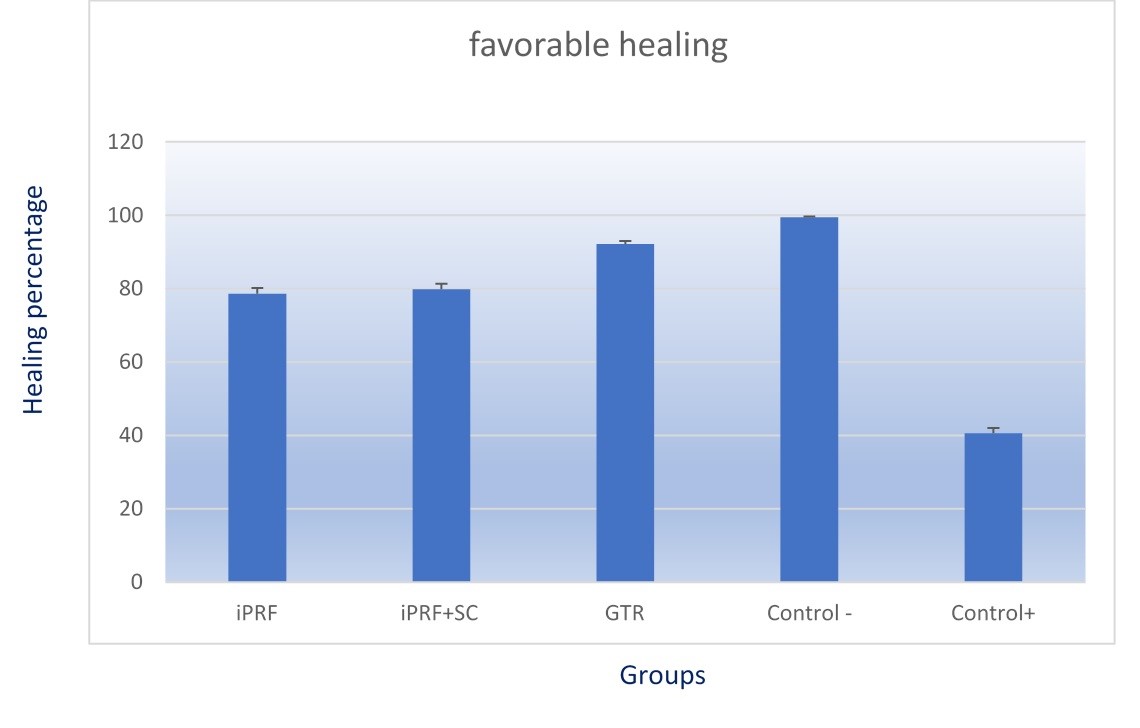
The histologic observations were performed by a laboratory technician using a projection microscope (BX50, Olympus Optical, Japan), and the images were captured (DP25, Olympus). All the data were collected and analysed by an independent investigator to reduce bias and errors. Histological assessment was conducted on tooth samples to evaluate different types of resorption (surface, inflammatory, and replacement resorption) and the repair of normal PDL (8). Areas with pathological resorption (inflammatory and replacement resorption) were classified as unfavorable healing, while areas with non-pathological or surface resorption were identified as favorable healing.
A histomorphometric analysis was then conducted by random cross-sections from each tooth. The images of the sections magnified at forty times were analyzed and the percentage occurrence of periodontal healing and root resorption was calculated with Pro-image analysis software (Olymplus, Japan). Briefly, the area of periodontal healing/resorption in one section could be enclosed by drawing one free line, and this specific area could be calculated automatically by the software. The frequency of each resorption type was calculated and provided an average percentage per tooth and group.
Statistical Methods
Descriptive data were represented by mean, standard deviation, graphs, and statistical tables. The chi-square test was employed for analyzing radiographic data. For the analysis of histologic data, the percentage of normal PDL and resorption in histopathological images were utilized. Based on the Kolmogorov-Smirnov test, the data was not normally distributed, and so the Kruskal-Wallis test was employed to compare each of the variables among the groups and Mann-Whitney U test was used for pairwise comparison. The data were analyzed using SPSS statistical software version 20. The significance level of all tests was considered 0.05%.

{kind=link}
{kind=link}
{kind=link}