Baseline data
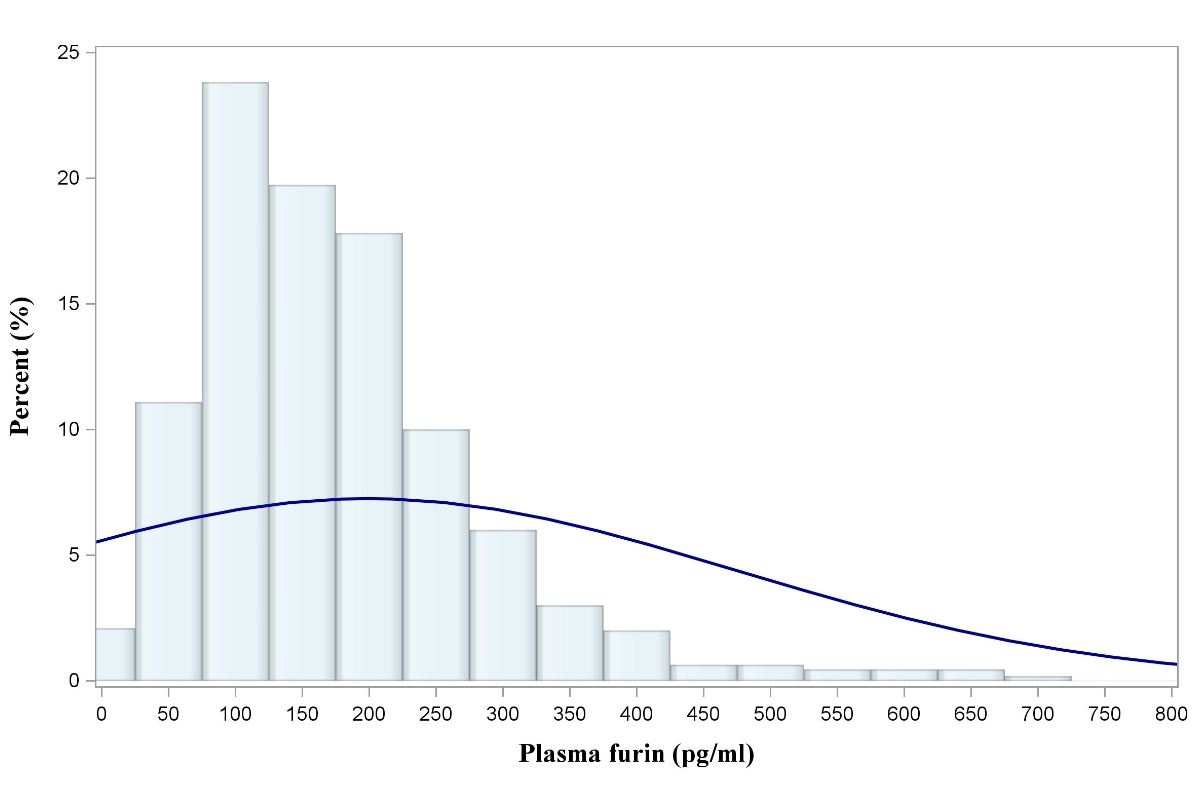
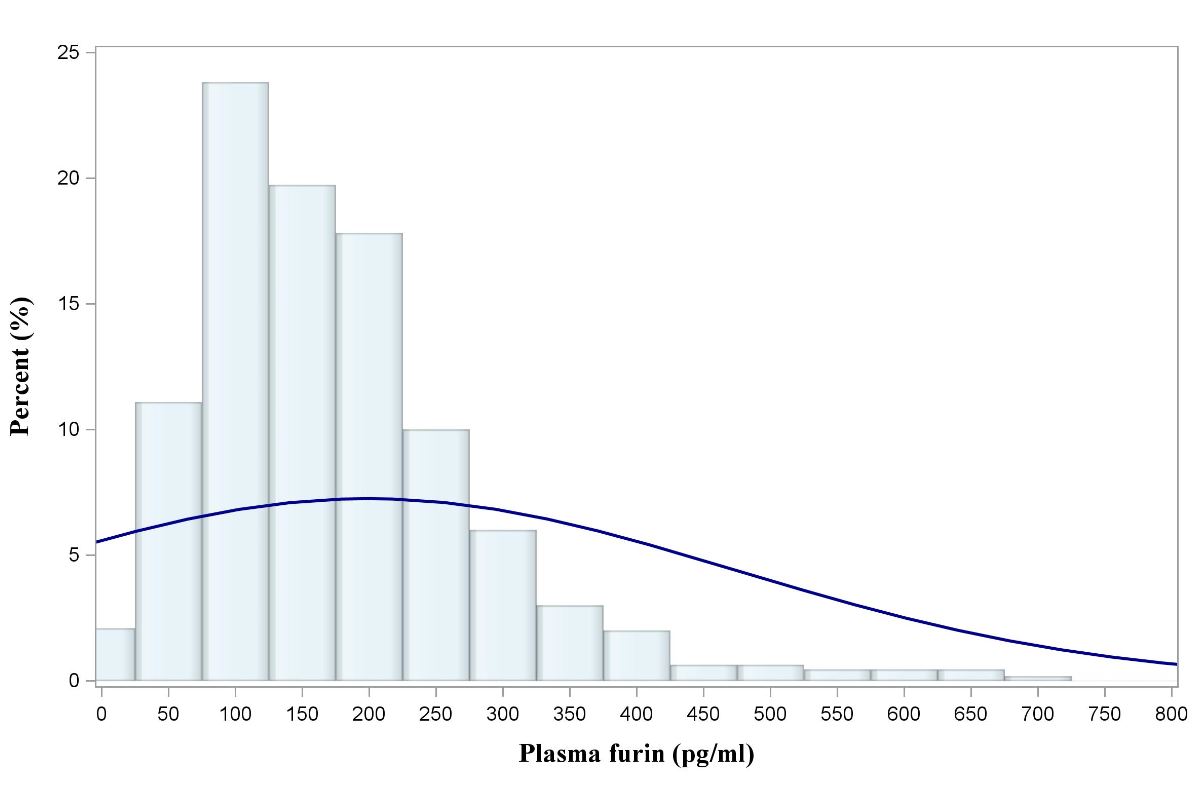
The mean age of 1,100 study participants was 61 ± 13 years; 77% were male. The distribution of plasma furin is left-skewed (sFigure 1). The median plasma furin levels were 156.6 (interquartile range, 102.4-228.8) pg/ml. There was no significant difference between male and female patients (158.5 [103.4-226.9] pg/ml for the male versus 145.9 [93.1-233.6] pg/ml for the female; P= 0.360), between diabetic and non-diabetic patients [160.9 (104.2-231.0] pg/ml for the diabetic versus 155.1 [101.6-224.9] pg/ml for the non-diabetic; P= 0.535), between hypertensive and non-hypertensive patients (154.0 [101.7-222.6] pg/ml for the hypertensive versus 160.8 [103.0-232.1] pg/ml for the non-hypertensive; P= 0.233) and between STEMI and non-STEMI patients (160.7 [105.3-231.4] pg/ml for STEMI versus 147.2 [94.9-220.1]pg/ml for NSTEMI; P=0.079).
sFigure1. Distribution of Plasma furin in our population.
Association between plasma furin levels and clinical parameters
The baseline characteristics of the study population listed in Table 1. AMI patients were divided into 3 groups according to tertile of plasma furin (≤117.5pg/ml, 117.5-200pg/ml, ≥200pg/ml). Slightly increase of mean cTNT were in patients with higher furin levels (P = 0.016). There is no significant increase of NT-proBNP as furin increases (Table 1).
Table 1. Baseline variables according to tertile of plasma furin in AMI patients.
|
|
Plasma furin (pg/mL)
|
P
value
|
|
|
Overall
|
≤117.5
|
117.5-200
|
≥200
|
|
Patients, n
|
1100
|
356
|
374
|
370
|
|
|
Anterior MI, n (%)
|
313 (29.6%)
|
100 (29.1%)
|
116 (32.4%)
|
97 (27.2%)
|
0.300
|
|
STEMI, n (%)
|
747 (69.6%)
|
231 (66.8%)
|
256 (70.7%)
|
260 (72.2%)
|
0.265
|
|
Age, year
|
61.0 (13.4)
|
60.8 (13.8)
|
61.6 (13.0)
|
60.7 (13.4)
|
0.489
|
|
Male, n (%)
|
817 (77.0%)
|
262 (75.9%)
|
275 (76.6%)
|
280 (78.4%)
|
0.718
|
|
Current smoker, n (%)
|
370 (41.9%)
|
127 (44.1%)
|
116 (38.5%)
|
127 (34.1%)
|
0.345
|
|
Medical history, n (%)
|
|
|
|
|
|
|
Diabetes mellitus
|
394 (37.1%)
|
122 (35.7%)
|
140 (38.8%)
|
132 (36.9%)
|
0.690
|
|
Hypertension
|
456 (43.2%)
|
150 (44.0%)
|
159 (44.5%)
|
147 (41.2%)
|
0.624
|
|
MI
|
45 (4.1%)
|
14 (3.9%)
|
13 (3.5%)
|
18 (4.9%)
|
0.623
|
|
CKD
|
20 (1.9%)
|
8 (2.4%)
|
7 (2.0%)
|
5 (1.4%)
|
0.654
|
|
AF
|
10 (0.9%)
|
4 (1.1%)
|
4 (1.1%)
|
2 (0.5%)
|
0.648
|
|
LIPID
|
121 (11.0%)
|
40 (11.2%)
|
38 (10.2%)
|
43 (11.6%)
|
0.828
|
|
HF
|
5 (0.5%)
|
4 (1.1%)
|
0 (0.0%)
|
1 (0.3%)
|
0.090
|
|
Clinical assessment
|
|
|
|
|
|
|
BMI, kg/m2
|
25.3 (3.6)
|
25.4 (3.8)
|
25.5 (3.7)
|
24.9 (3.3)
|
0.079
|
|
HBA1C, %
|
6.7 (1.6)
|
6.7 (1.6)
|
6.8 (1.6)
|
6.6 (1.6)
|
0.465
|
|
Glucose, mmol/ L
|
8.5 (3.9)
|
8.3 (3.5)
|
8.4 (4.0)
|
8.7 (4.3)
|
0.944
|
|
Cr, umol/ L
|
78.5 (68.0, 94.7)
|
79.1 (67.6, 95.6)
|
78.1 (67.6, 93.9)
|
78.0 (68.7, 93.8)
|
0.912
|
|
LVEF, %
|
50.5 (9.0)
|
51.0 (9.0)
|
50.1 (9.3)
|
50.5 (8.7)
|
0.509
|
|
cTNT, pg/mL
|
1.8 (0.5, 4.9)
|
1.4 (0.4, 3.9)
|
1.7 (0.5, 4.6)
|
2.1 (0.6, 6.2)
|
0.016
|
|
NT-proBNP, pg/mL
|
1566(668, 3929)
|
1427 (610, 3490)
|
1587 (712, 4098)
|
1645 (709, 4049)
|
0.361
|
|
HR
|
77.6 (14.9)
|
76.5 (13.5)
|
77.3 (14.2)
|
78.8 (16.7)
|
0.591
|
|
CHOL, mmol/ L
|
4.3 (1.1)
|
4.2 (1.1)
|
4.4 (1.1)
|
4.2 (1.1)
|
0.601
|
|
TRIG, mmol/ L
|
1.3 (0.9, 1.8)
|
1.3 (0.9, 1.8)
|
1.3 (1.0, 1.9)
|
1.3 (0.9, 1.8)
|
0.453
|
|
LDL, mmol/ L
|
2.7 (0.9)
|
2.6 (0.9)
|
2.7 (1.0)
|
2.7 (0.9)
|
0.588
|
|
HDL, mmol/ L
|
1.1 (0.3)
|
1.1 (0.3)
|
1.1 (0.3)
|
1.1 (0.3)
|
0.771
|
|
AST, U/ L
|
45.6 (24.5, 108.3)
|
42.1 (24.3, 91.1)
|
43.9 (24.4, 100.3)
|
52.0 (26.6, 132.7)
|
0.112
|
|
ALT, U/ L
|
30.8 (19.6, 52.5)
|
31.6 (19.4, 51.7)
|
30.7 (19.7, 51.1)
|
31.1 (19.6, 55.1)
|
0.898
|
|
GGT, U/ L
|
29.1 (19.3, 47.9)
|
28.4 (19.3, 48.5)
|
28.9 (19.3, 47.1)
|
29.7 (19.4, 51.0)
|
0.772
|
|
PT, s
|
14.1 (2.0)
|
14.0 (2.1)
|
14.0 (1.3)
|
14.3 (2.3)
|
0.114
|
|
APTT, s
|
39.4 (35.3, 46.8)
|
38.8 (35.3, 45.6)
|
39.3 (35.1, 45.9)
|
39.9 (35.4, 51.5)
|
0.304
|
|
DDIMER, ng/ L
|
0.4 (0.3, 0.8)
|
0.4 (0.3, 0.8)
|
0.4 (0.3, 0.8)
|
0.4 (0.3, 0.9)
|
0.653
|
|
Medications, n (%)
|
|
|
|
|
|
|
Aspirin
|
1021 (96.3%)
|
334 (97.1%)
|
347 (96.7%)
|
340 (95.2%)
|
0.392
|
|
ACEI/ARB
|
434 (40.9%)
|
146 (42.4%)
|
158 (44.0%)
|
130 (36.4%)
|
0.093
|
|
Statin
|
1033 (97.5%)
|
338 (98.3%)
|
351 (97.8%)
|
344 (96.4%)
|
0.251
|
|
DIURETIC
|
572 (52.0%)
|
186 (52.2%)
|
193 (51.6%)
|
193 (52.2%)
|
0.996
|
|
CABLOCKER
|
121 (11.0%)
|
45 (12.6%)
|
41 (11.0%)
|
35 (9.5%)
|
0.394
|
|
BETABLOCKER
|
528 (48.0%)
|
187 (52.5%)
|
178 (47.6%)
|
163 (44.1%)
|
0.070
|
|
GLP1
|
22 (2.0%)
|
6 (1.7%)
|
8 (2.1%)
|
8 (2.2%)
|
0.875
|
|
INSULIN
|
531 (48.3%)
|
158 (44.4%)
|
182 (48.7%)
|
191 (51.6%)
|
0.146
|
|
DPP4
|
49 (4.5%)
|
15 (4.2%)
|
16 (4.3%)
|
18 (4.9%)
|
0.895
|
Data are presented as mean (SD), median (interquartile range) or numbers (percentages). ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blocker; BMI, body mass index; cTNT, cardiac troponin T; eGFR, estimated Glomerular Filtration Rate; LVEF, left ventricular ejection fraction; MI, myocardial infarction; STEMI, ST-elevation myocardial infarction.
In Spearman correlation analysis, the results showed that log furin did not correlate with age, blood glucose, HbA1c, left ventricular ejection fraction, log eGFR, log cTNT, log CKMB, log NT–proBNP (sTable 1).
sTable 1. Spearman correlation analysis of log furin with covariates.
|
Age
|
Glucose
|
HbA1c
|
Log eGFR
|
LVEF
|
Log CKMB
|
Log cTNT
|
Log NT-proBNP
|
|
Log Furin
|
0.007
|
0.022
|
-0.007
|
0.035
|
-0.003
|
0.051
|
0.065
|
0.018
|
Kaplan-Meier analysis
Over a median follow-up of 31 month, 133 cases of cardiovascular death, 37 cases of non-cardiovascular death, 26 cases of recurrent non-fatal MI, 22 cases of non-fatal stroke and 27 cases of hospitalization for heart failure occurred in this population. Kaplan-Meier survival analysis results suggested that furin was not associated with composite CV outcomes (Figure 1).
Figure 1. Kaplan–Meier analysis of MACE rates in AMI patients according to different furin category
COX regression analysis of end points
Cox regression analysis indicated that Increasing plasma furin levels was not associated with increasing risk of MACE (HR: 1.01; 95% CI: 0.93-1.06; P=0.807). In addition, for each endpoint of CV death, non-fatal MI, non-fatal stroke, non-CV death, all death or hospitalization for HF, our findings showed that plasma furin was not associated with all these end point except possible recurrent non-fatal MI (HR: 1.09; 95% CI: 1.01-1.17; P = 0.022). (Table 2)
Table 2. Every 50 unit increase of furin on cardiovascular outcomes
|
|
|
Unadjusted
|
|
Model 1
|
|
Model 2
|
|
|
|
Event/No
|
HR (95% CI)
|
P value
|
HR (95% CI)
|
P value
|
HR (95% CI)
|
P value
|
|
MACE
|
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
60/356
|
1.12 (0.80, 1.56)
|
0.519
|
1.18 (0.84, 1.66)
|
0.338
|
1.41 (0.91, 2.17)
|
0.125
|
|
|
Median (117.5-200)
|
57/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
64/370
|
1.04 (0.74, 1.46)
|
0.824
|
1.08 (0.77, 1.53)
|
0.655
|
1.20 (0.76, 1.90)
|
0.433
|
|
|
50 pg/mL increase
|
181/1100
|
1.01 (1.00, 1.03)
|
0.084
|
1.02 (1.00, 1.03)
|
0.030
|
1.01 (0.96, 1.06)
|
0.807
|
|
|
CV death
|
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
46/356
|
1.17 (0.77, 1.78)
|
0.465
|
1.21 (0.79, 1.86)
|
0.376
|
1.29 (0.75, 2.22)
|
0.350
|
|
|
Median (117.5-200)
|
42/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
45/325
|
1.10 (0.72, 1.67)
|
0.661
|
1.20 (0.78, 1.84)
|
0.410
|
1.02 (0.57, 1.83)
|
0.939
|
|
|
50 pg/mL increase
|
133/1100
|
1.01 (1.00, 1.03)
|
0.078
|
1.02 (1.00, 1.04)
|
0.013
|
0.99 (0.92, 1.06)
|
0.709
|
|
|
Non-fatal MI
|
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
7/356
|
1.16 (0.41-3.30)
|
0.786
|
1.20 (0.42, 3.45)
|
0.734
|
1.68 (0.36, 7.90)
|
0.509
|
|
|
Median (117.5-200)
|
7/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
12/370
|
1.67 (0.66, 4.25)
|
0.280
|
1.73 (0.68, 4.45)
|
0.253
|
5.12 (1.24, 21.2)
|
0.024
|
|
|
50 pg/mL increase
|
26/1100
|
1.02 (0.98, 1.07)
|
0.394
|
1.02 (0.98, 1.07)
|
0.316
|
1.09 (1.01, 1.17)
|
0.022
|
|
|
Non-fatal Stroke
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
7/356
|
1.04 (0.38, 2.86)
|
0.945
|
0.99 (0.35, 2.74)
|
0.976
|
1.34 (0.41, 4.40)
|
0.625
|
|
|
Median (117.5-200)
|
8/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
7/370
|
0.88 (0.32, 2.43)
|
0.806
|
0.83 (0.29, 2.41)
|
0.731
|
0.62 (0.15, 2.65)
|
0.521
|
|
|
50 pg unit increase
|
22/1100
|
0.92 (0.76, 1.11)
|
0.389
|
0.91 (0.74, 1.12)
|
0.358
|
0.85 (0.64, 1.14)
|
0.277
|
|
|
Hospitalized HF
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
10/356
|
1.05 (0.44, 2.53)
|
0.908
|
1.08 (0.45, 2.60)
|
0.860
|
1.85 (0.53, 6.39)
|
0.333
|
|
|
Median (117.5-200)
|
10/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
7/370
|
0.71 (0.27, 1.85)
|
0.479
|
0.74 (0.28, 1.94)
|
0.540
|
1.71 (0.48,6.10)
|
0.405
|
|
|
50 pg/mL increase
|
27/1100
|
0.99 (0.91, 1.09)
|
0.862
|
0.99 (0.90, 1.09)
|
0.876
|
1.03 (0.94,1.14)
|
0.490
|
|
|
Non-CV death
|
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
16/356
|
1.68 (0.76, 3.71)
|
0.197
|
1.88 (0.85, 4.15)
|
0.121
|
1.70 (0.60, 4.79)
|
0.316
|
|
|
Median (117.5-200)
|
10/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
11/370
|
1.11 (0.47, 2.61)
|
0.817
|
1.15 (0.49, 2.71)
|
0.097
|
0.58 (0.14, 2.39)
|
0.449
|
|
|
50 pg/mL increase
|
37/1100
|
1.01 (0.99, 1.04)
|
0.305
|
1.02 (1.00, 1.05)
|
0.093
|
0.94 (0.75, 1.17)
|
0.561
|
|
|
All death
|
|
|
|
|
|
|
|
|
|
Low (≤117.5)
|
62/356
|
1.28 (0.89, 1.85)
|
0.191
|
1.36 (0.93, 1.98)
|
0.112
|
1.37 (0.85, 2.22)
|
0.195
|
|
|
Median (117.5-200)
|
52/374
|
Ref.
|
|
Ref.
|
|
Ref.
|
|
|
|
High (≥200)
|
56/370
|
1.11 (0.76, 1.62)
|
0.600
|
1.21 (0.83, 1.78)
|
0.327
|
0.94 (0.55, 1.59)
|
0.804
|
|
|
50 pg/mL increase
|
170/1100
|
1.02 (1.00,1.03)
|
0.025
|
1.02 (1.01, 1.04)
|
0.002
|
0.98 (0.92, 1.05)
|
0.548
|
|
Model 1 adjusted for age and sex;
Model 2 adjusted for model 1 plus eGFR, BMI, smoking, history of diabetes, hypertension or myocardial infarction, STEMI/non-STEMI.
Subgroup analysis
Subgroup analysis according to age, gender, BMI, history of smoking, diabetes, hypertension, types of MI (STEMI / NSTEMI), showed that the association between furin and MACE did not differ in these subgroups (figure 2).
Figure 2. Furin on cardiovascular outcomes subgroup patients.
Finally, we constructed univariable cox regression analysis to identify variables that may independently associated with MACE in our population (table 3). The results showed that NT–proBNP (P < 0.001), age (P < 0.001), creatinine (P < 0.001), cTnT (P = 0.001), blood glucose (P = 0.001), diabetes history (P = 0.010), CKD history (P=0.023) and STEMI (P = 0.039) were positively associated MACE. In contrast, LVEF (P < 0.001), usage of aspirin (P < 0.001), ACEI / ARB (P < 0.001) and women (P = 0.001) were negatively associated with MACE.
Table 3. Univariable predictors of MACE after MI in all study population
|
Predictors
|
Chi-Square
|
HR (95%CI)
|
P
|
|
NT-proBNP (1000 pg/ml greater)
|
240.4268
|
1.09 (1.08, 1.11)
|
<0.001
|
|
Age (year older)
|
120.0124
|
1.07 (1.05, 1.08)
|
<0.001
|
|
LVEF (1% greater)
|
94.6846
|
0.93 (0.91, 0.94)
|
<0.001
|
|
Creatinine(10 unit increase)
|
21.6745
|
1.02 (1.01-1.03)
|
<0.001
|
|
Aspirin (Yes/No)
|
14.0069
|
0.38 (0.23, 0.63)
|
<0.001
|
|
ACEI/ARB (Yes/No)
|
12.1239
|
0.57 (0.42, 0.78)
|
<0.001
|
|
cTNT (1 μg/L greater)
|
11.4552
|
1.03 (1.01, 1.04)
|
0.001
|
|
Glucose (1 mg/dL greater)
|
11.4426
|
1.05 (1.02, 1.07)
|
0.001
|
|
Male
|
10.3531
|
0.61 (0.45, 0.82)
|
0.001
|
|
Diabetes (Yes/No)
|
6.6461
|
1.45 (1.09, 1.93)
|
0.010
|
|
CKD (Yes/No)
|
5.1332
|
2.40 (1.13, 5.10)
|
0.023
|
|
STEMI
|
4.2433
|
1.36 (1.01, 1.82)
|
0.039
|
|
Hypertension (Yes/No)
|
2.6197
|
1.27 (0.95, 1.69)
|
0.106
|
|
Furin (50 pg/mL greater)
|
2.1521
|
1.01 (1.00, 1.03)
|
0.142
|
|
Hba1c (1 unit greater)
|
1.7690
|
1.07 (0.97, 1.19)
|
0.184
|
|
Statin (Yes/No)
|
0.0710
|
0.90 (0.40, 2.02)
|
0.790
|
{kind=link}
{kind=link}