In this retrospective study we were able to identify biomarkers predictive of recurrence of CSCR by the means of AI and ML methods. This research represents the first investigation addressing a fundamental clinical inquiry: determining which patients are prone to experiencing recurrence following an initial, spontaneously resolved episode of CSCR. In fact, recurrence of SRF is a negative prognostic factor on long-term visual outcomes causing RPE and PR alterations [20]. The gold standard treatment of PDT with verteporfin showed good efficacy on fluid resolution and preservation of functional visual acuity [11]. Therefore, it would be helpful to be able to predict which patients will experience recurrences in order to optimize follow-up schedule and promptly arrange treatment.
The current paper aims to identify optical coherence tomography (OCT)-derived parameters linked to CSCR recurrence, by means of Discovery® software (by RetinAI) for identifying and quantifying different SD-OCT biomarkers in CSRC.
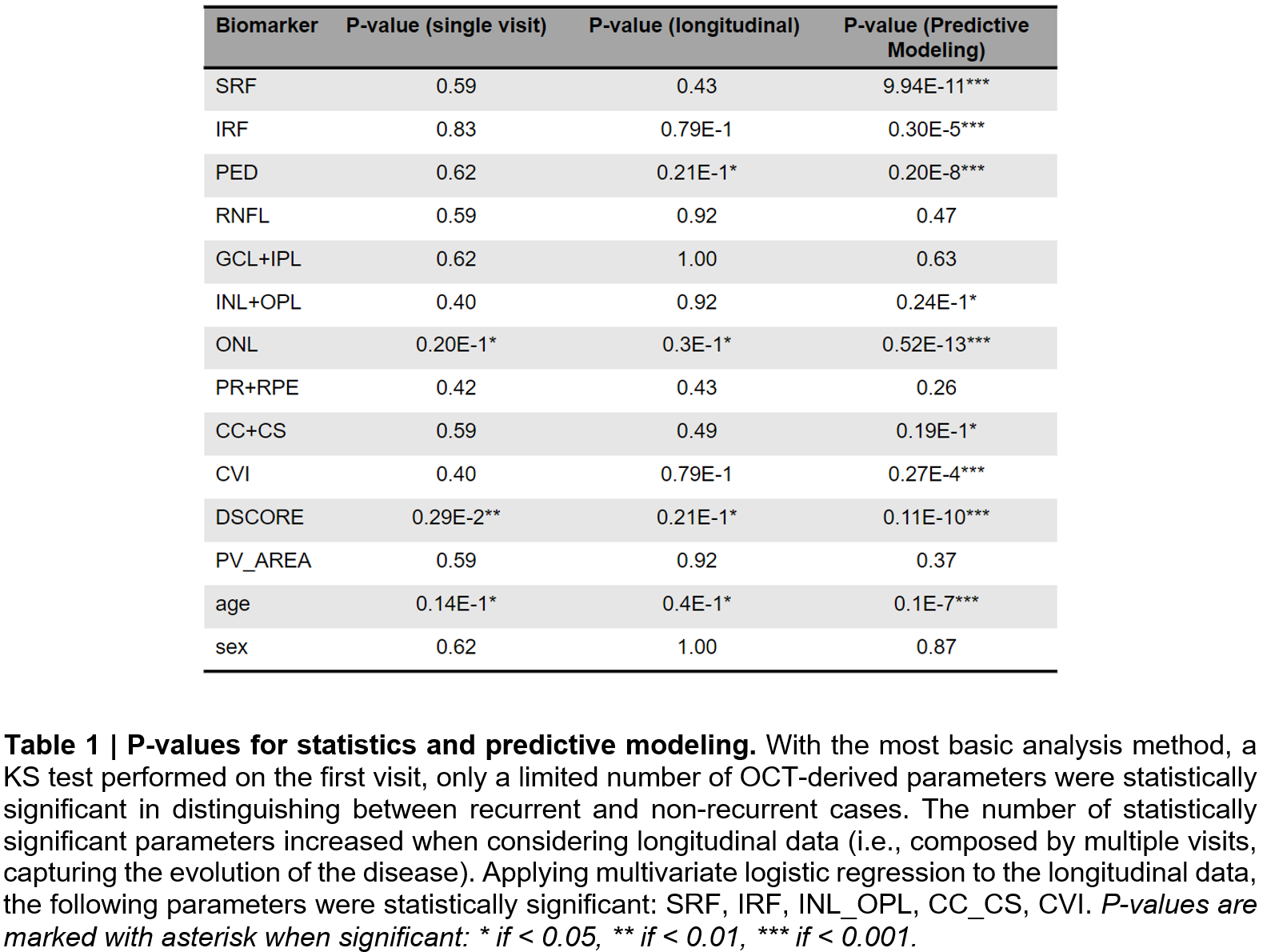
Our study identified nine OCT predictive biomarkers for the recurrence of CSCR, in particular, volume of Subretinal Fluid (SRF), volume of Intraretinal Fluid (IRF), area of Pigment Epithelial Detachment (PED) in the central, pericentral and peripheral areas, and thicknesses of the following 6 layers (or combinations thereof) in the central area (C1): Chorio-Capillaris and Choroidal Stroma (CC + CS), Photo-Receptors and Retinal Pigment Epithelium (PR + RPE), Outer Nuclear Layer (ONL), Inner Nuclear Layer and Outer Plexiform Layer (INL + OPL), Ganglion Cell Layer and Inner Plexiform Layer (GCL + IPL), Retinal Nerve Fiber Layer (RNFL).
Three additional biomarkers were extracted: the Choroidal Vascularity Index (CVI), a score estimating disruption or the PR + RPE layer (DSCORE), and an estimation of the area of the largest Choroidal Pachyvessel (PV_AREA).
The multivariate logistic regression to the longitudinal data, demonstrated that the following parameters were statistically significant: SRF, IRF, INL_OPL, CC_CS, CVI (as shown in Fig. 4). Therefore, we showed that all these parameters were related to CSCR recurrence.
Recently, imaging biomarkers associated with acute and chronic CSCR were analyzed with an AI software [25]. The authors found a significant increase in thickness in both outer retinal layers (ONL, PR and RPE layer) and inner retinal layers (INL and GCL), and SRF in patients with acute CSCR compared to chronic CSCR at baseline. However, in our study we identified more parameters independently of the type of CSCR, which might better reflect the real-world practice. Also, Xu et al. analyzed recurrences in CSCR patients with six different models of AI and ML [26].
Imaging has become a key factor in clinical practice since the introduction of fast, high resolution machines. Therefore, the volume of data to analyze increased and new systems of automatic analysis are now available. The application of AI and ML models now becomes the next step forward in the optimization of data analysis mostly to predicting outcomes.
Nowadays, by the word 'biomarker', scientists refer to morphological and structural changes that can provide important information on the stage of a disease. The search for new biomarkers in retinal diseases has been a field of great interest in recent years. This research has been driven by the need for earlier and more accurate diagnosis, better prognostication and the development of target therapies.
Many researches have been carried out on biomarkers in retinal diseases such as age-related macular degeneration and diabetic macular edema. The predictive role of retinal biomarkers in CSCR has been reported in a recent study [27]. In particular, changes in central macular thickness and subfoveal choroidal thickness were associated to the resolution of CSCR, while the amount of SRF to the visual acuity outcomes. Moreover, the morphology of the retinal layers, such as ONL thinning, PR layer elongation, ELM and ellipsoid zone disruption was previously associated with longer duration of SRF and worse visual acuity [17, 28, 29].
The definition and validation of predictive biomarkers for central serous chorioretinopathy recurrence is crucial for physicians in daily clinical practice for several reasons. Firstly, predictive biomarkers may allow early diagnosis of individuals at risk of CSCR recurrence. Early diagnosis allows for early intervention and management, potentially preventing serious complications and preserving vision. Furthermore, biomarkers could help tailor treatment strategies to individual patient profiles.
By identifying patients most likely to relapse, clinicians can offer customized treatment plans.
By understanding the likelihood of recurrence, physicians can set realistic expectations and plan for long-term management, and by identifying high-risk patients, physicians can optimize the use of resources by defining proper follow-up in relation to the likelihood of recurrence.
Biomarkers contribute to the advancement of research and development efforts in understanding the underlying mechanism and risk factors associated with CSCR recurrence. They can lead to the development of more effective therapies and preventive strategies.
Despite the promising results linking OCT-derived biomarkers with a future recurrence of CSCR, our study was subject to several limitations that warrant discussion.
One of the primary challenges was the variability in the number of visits of each patient, particularly pronounced among chronic or recurrent CSCR cases since recurrent patients are examined more often and for longer periods. Our dataset also presented a wide variability in terms of Subretinal Fluid (SRF) volumes. SRF can range from minimal (around 10 nL) to significant (up to 10,000 nL), complicating the identification and categorization of CSCR episodes. Despite a general definition of a CSCR episode as an accumulation of SRF which is followed by drying up of the fluid, the diverse manifestations based on the patient’s SRF range make it challenging to clearly distinguish between multiple occurrences and a single episode. This made it challenging even for medical professionals with decades of experience in the disease, underlining the complexity of the labeling task.
In our study, a particularly significant limitation was the binary labeling system used to classify CSCR cases as either recurrent or non-recurrent. This classification framework, while straightforward and appropriate given the size of our dataset, proved insufficient handling the inherent complexities and ambiguities of certain patient cases. Especially challenging was the accurate categorization of chronic patients, which are characterized by fluctuating levels of SRF. Applying our labeling system led to chronic patients being labeled as recurrent cases, despite the nuances in their condition that might suggest a more complex categorization. This subgroup, characterized by SRF volumes that persistently remain above zero, likely represents a distinct clinical picture. In a few cases, chronic patients were excluded from our analysis. Their exclusion, while necessary for the integrity of our current analysis, highlights the limitations of a binary classification system which future work could address via multi-label annotation.
Additionally, an intrinsic limitation of our study is that some patients who were classified as non-recurrent (based on the data available at the time the dataset was collected), might have experienced a CSCR episode post-data collection. This potential for future occurrences not captured in our current dataset underscores the dynamic nature of CSCR and the challenges inherent in predicting its course.
Looking at the correlation matrix we found that ONL thickness strongly correlated with D_SCORE, consistently with what is reported in the literature [30, 31].
Fitting one biomarker at a time, the logistic regression results in a pseudo R-squared (~ proportion of variance explained) that is at maximum 3.0%. Then, the Logistic Regression (LR) model fitted with all our parameters at the same time explained only 8.7% of the variance among patients.
Finally, our approach did not make explicit use of the time dimension inherent in our data. Leveraging methods able to consider the evolution of biomarkers over time might enable the prediction of CSCR recurrence and pave the way for translational medical applications.
Our analysis revealed correlations between several biomarkers and CSCR recurrence. Applying logistic regression (LR) to all biomarkers explained 8.7% of the variance among patients. Despite the usefulness of these results in elucidating the importance of each biomarker, this suggests a limited capacity of these models to adequately capture the complexities of CSCR recurrence.
Looking ahead, significant work remains before these models can be used in clinical applications. A critical unexplored aspect in our current approach is the incorporation of the time dimension in data analysis. Time-series analysis could significantly improve predictive accuracy, opening avenues for practical medical applications. However, advanced modeling techniques like deep learning, while promising enhanced predictive performance, often reduce the model's explainability, a critical factor in clinical settings. Therefore, our future research will aim to balance sophisticated modeling capabilities with the clarity and transparency essential for clinical applicability.
{kind=link}