Foreign-body aspiration accounts for high morbidity if the diagnosis is delayed or missed. Mortality also is reported in children, especially between ages 12 months to 3 years. (2) Most children under the age of 3 years tend to mull over most particles in their mouths, they also have flawed nibbling habits and premature swallowing coordination which makes them more prone for a FBA. Children are more susceptible to some FBA complications due to immature defense mechanisms. (6) Often the presentation and initial radiological findings are vague, which impedes the early diagnosis. An alleged episode of choking and severe cough is a critical evidence in the diagnosis of FB aspiration.
In our study, choking (5.40%) and hemoptysis (2.70%) were seen in limited cases. The most common symptoms in patients who presented early (< 1 week) were tachypnea (58.8%), wheeze (47.05%) and wet cough (41.1%). In cases of delayed presentation (>1 week) majority complained of fever (65%) and dry cough (45%). It was found that the delay in presentation was mostly due to unintentional aspiration by child unnoticed by parents, vague clinical history, lack of respiratory symptoms, unwillingness by the treating physician for getting a chest X ray and delayed referral. It was noted that the duration of treatment at the local hospital was directly proportional to the duration of admission later for effective management.
Unlike adults, toddlers do not have clear recall of FBA, thus the diagnosis is most often dependent on the mother’s history, clinical findings such as onset and duration of symptoms and suspicion. Chest x -ray is the most common investigation done in these cases and majority of the time chest- x rays are normal (fig 4).
The typical findings on chest radiograph which is diagnostic is unilateral lung hyperinflation, collapse, consolidation of one lung and mediastinal shift. Many authors in their study have reported percentage of normal chest X -ray around 20-42 % (7, 8). In our study normal chest x-ray was found in 39% of patients. Normal chest X-ray is accepted in early phase as most aspirated foreign bodies are vegetative in nature and cannot be seen on chest x ray.
Later, when the organic substance swells with inflammation it occludes the bronchus completely and typical chest x-ray findings appear (fig 5).
On the contrary, most of the metallic objects are relatively radiolucent and easily picked up on chest X ray and aids clinicians in early diagnosis of FBA (fig 6) .
Recently Computerized tomography (CT) has been introduced as a noninvasive procedure in the diagnosis of FBA, but it is known to show false positive results and also has radiation hazards associated with it. (9, 10, 11)
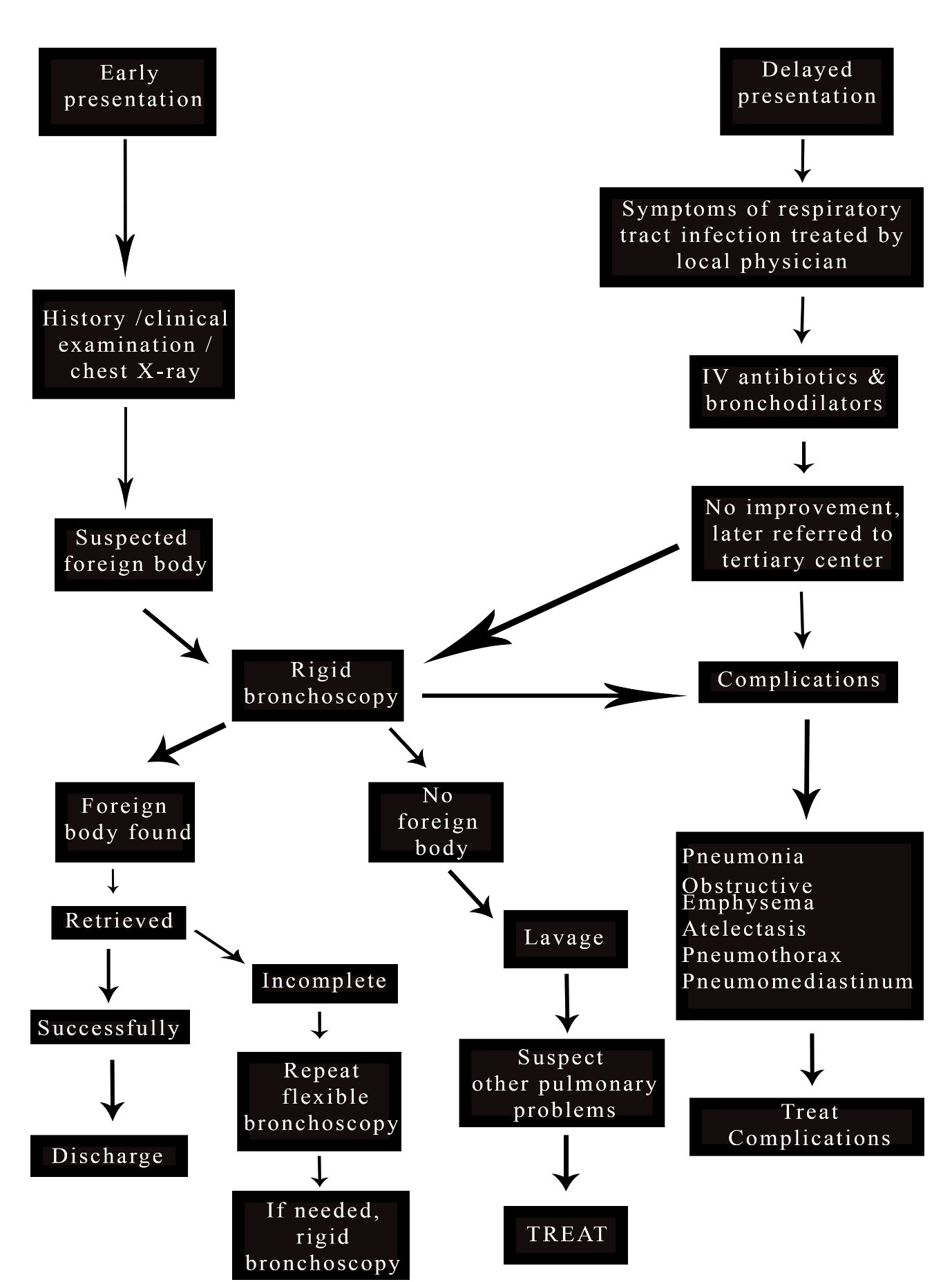
Various other diagnostic modalities have been reported to be effective, rigid bronchoscopic inspection being the gold standard (12). It is an invasive procedure done under general anesthesia and has some morbidity (7). Some authors suggested that flexible bronchoscopy is a useful procedure for foreign body retrieval from infants and children with a 91.3% success rate (13). Rigid or flexible bronchoscopy especially in pediatric patients remains a controversy and depends on the institute protocol. In our study all patients underwent rigid bronchoscopy initially. In 4 cases where incomplete retrieval was done, flexible bronchoscopy was used for inspection followed by a rigid bronchoscopy for retrieval.
In our study nature of foreign body aspirated were mostly organic 81.1% and inorganic foreign body accounted for 18.9%. Routinely found FB was peanut being present in 43.24% patients.
Many authors have reported the disparity between aspiration and hospital admission was more than 24 hours and even after that there was a delay in diagnosis (14). Some of the larger reviews have documented delays ranging from 20-40% of the patients reviewed (15). In this present study, 54.04% of the patients reviewed had delayed presentation.
Delay in presentation were due to unintentional aspiration by child unnoticed by parents, vague clinical history, lack of respiratory symptoms, the unwillingness of the treating physician for getting a chest X ray and late referral. The severity of symptoms depends on the degree of obstruction of the tracheobronchial tree so it can be complete or incomplete and site of obstruction. If there is complete obstruction these patients are referred early. Delay usually occurs in patients with incomplete obstruction with normal chest X ray. A lack of history of inhalation most commonly led to delayed presentation and resulted in various respiratory complications like pneumonia, obstructive emphysema, atelectasis, pneumothorax and pneumomediastinum (16-17). Literature reveals there is a 7% incidence of pre hospital deaths in cases of foreign body aspiration (16).
Another factor that causes preoperative complications associated with FBA is the lack of standard treatment guidelines and management procedures. (6)
Based on our study, we have developed an algorithm for management on the basis of outcomes.
{kind=link}