Despite advancements in surgery and chemotherapy, colon cancer (CC) remains a highly fatal cancer with a poor prognosis [22]. Various biological processes have been implicated in the tumorigenesis and progression of CC, including cellular senescence [23].
Cellular senescence, traditionally considered a protective mechanism against cancer development, is a state of durable cell proliferative arrest [24, 25]. However, recent research has highlighted the complex relationship between cell senescence and tumor occurrence/development, identifying evasion of senescence as a necessary condition for cells to become cancerous [26, 27]. Long non-coding RNAs (lncRNAs) have been found to play important roles in multiple processes in CC. Prognostic models based on lncRNA signatures have been identified in various malignancies, including prostate cancer [28], lung cancer [29], and breast cancer [30].
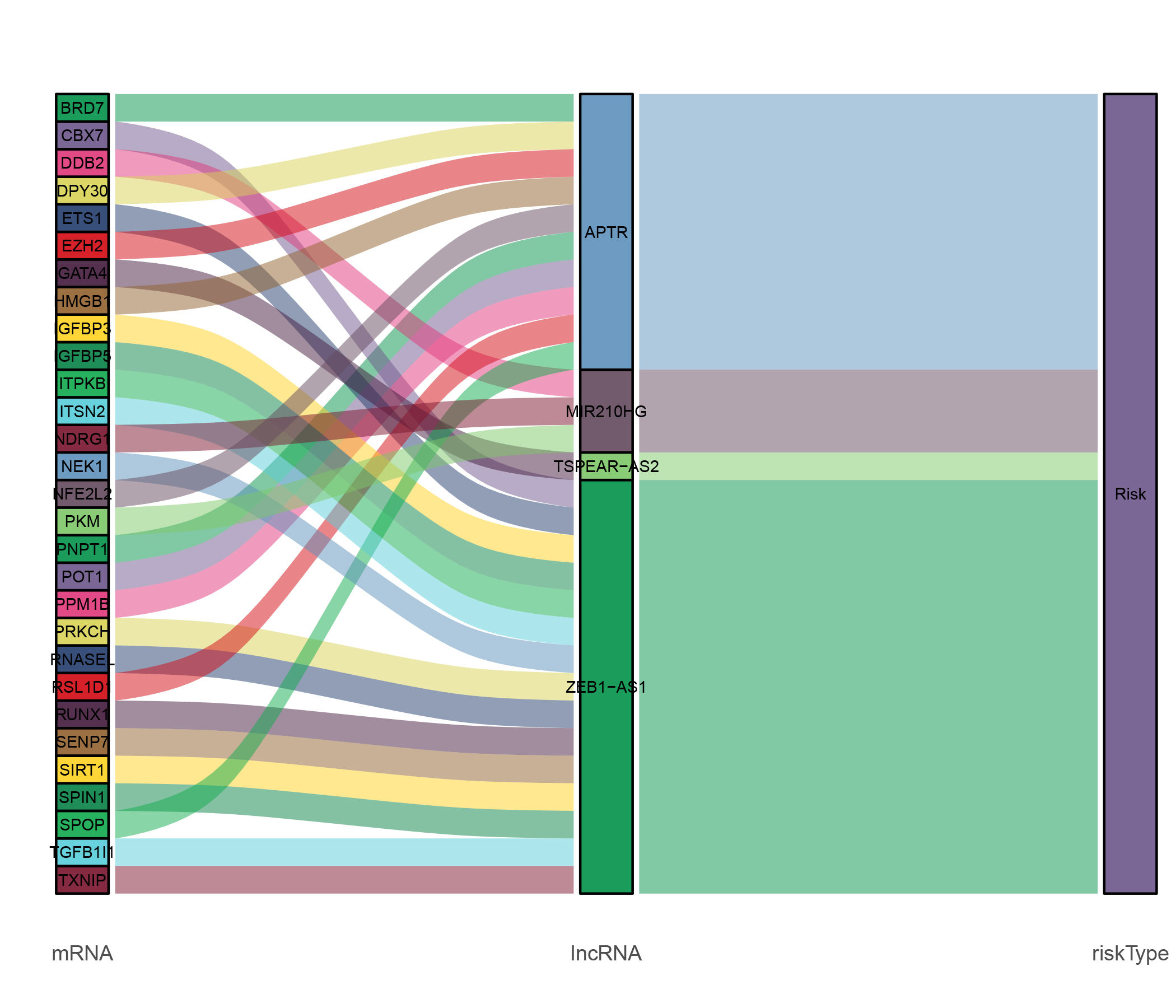
In CC, several lncRNA-based prognostic risk models have also gained attention. However, comprehensive analysis of prognostic models based on senescence-related lncRNAs (SRLs) in CC is still lacking [31]. In this study, we report the development of an SRL signature in CC patients, consisting of four lncRNAs (MIR210HG, TSPEAR-AS2, APTR, and ZEB1-AS1). Implicated in various biological processes, including cell senescence, these lncRNAs may have prognostic implications in CC through their dysregulation. By incorporating these SRLs into a risk model, we aim to provide a comprehensive and accurate tool for predicting the prognosis of CC patients.
Insights into the functional roles of the SRLs identified in this study in various malignant tumors have been provided by existing research. For instance, MIR210HG has been shown to influence the aggressiveness of endometrial cancer and breast cancer cells [32, 33]. In breast cancer, the C-myc/TSPEAR-AS2 axis has been implicated in promoting metastasis in a GLUT1-dependent manner [34]. The lncRNA APTR has been found to target the p21 promoter and promote leiomyoma cell proliferation through the Wnt/β-catenin pathway [35]. Additionally, ZEB1-AS1, a crucial cancer-related lncRNA, has been associated with advanced stage and poor survival in CC patients and found to be highly expressed in colon adenocarcinoma (COAD) tissues [36, 37].
To fully understand the specific roles and underlying mechanisms of these SRLs in CC, further research is needed. The validation of the prognostic value of the SRL-based risk model in clinical settings is also important. The precise mechanisms by which these SRLs contribute to tumorigenesis and progression in CC could be elucidated through large-scale clinical studies and functional experiments. Such research could not only enhance our understanding of the biology of CC, but also potentially pave the way for the development of novel targeted therapies and personalized treatment approaches based on the SRL-based risk model.
GO enrichment analysis and GSVA were conducted using the identified differentially expressed genes (DEGs) to compare the low- and high-risk groups, in order to explore the biological significance of the SRL signature in CC patients. The analysis revealed several enriched GO terms related to cellular processes and pathways. The SRL signature was found to be primarily enriched in GO terms such as “cell junction assembly,” “axonogenesis,” “RNA catabolic process,” and “positive regulation of cellular catabolic process”. This suggests that the identified SRLs may play important roles in these biological processes in CC.
Furthermore, GSVA revealed differences in pathway enrichment between the low- and high-risk groups. Specifically, there were significant differences in the “HYPOXIA,” “KRAS_SIGNALING_DN,” and “TNFA_SIGNALING_VIA_NFKB” pathways [38]. The KRAS oncogene is known to be frequently mutated in colorectal cancer, including CC, and is associated with poor prognosis [39, 40]. Hypoxia, on the other hand, has been implicated in cellular malignancy and has a significant impact on cell senescence [41, 42]. Exposure of senescent cells to hypoxic conditions activates the AMPK pathway, which in turn inhibits the mTOR/NF-κB signaling pathway.
Moreover, compounds that mimic hypoxia have been shown to reduce senescence-associated secretory phenotype (SASP) and improve the efficacy of chemotherapy and the status of aging mice [43].
A clinical practicality nomogram that incorporates age, T stage, N stage, M stage, and the SRL-based risk score was developed to improve the sensitivity of the SRL-based risk model for identifying patients with poor prognosis in CC. It was found in our study that the SRL signature was a stronger predictor of overall survival (OS) in CC patients compared to other factors. In estimating patient outcomes, the developed nomogram demonstrated satisfactory performance. Patients with high SRL risk scores had worse prognoses, and this was confirmed in the validation cohort. In fact, the average area under the curve (AUC) exceeded 0.7 in the validation cohort. The calibration curve indicated that the C-index of our nomogram reached 0.843 (95% CI = 0.801–0.884), suggesting that the nomogram can effectively predict OS based on individual patient conditions in CC.
Kaplan-Meier analysis and chemotherapy sensitivity analysis were also conducted. The results of the chemotherapy sensitivity analysis indicate that the SRL-based prognostic signature may contribute to a better understanding of the molecular mechanisms underlying CC pathogenesis and provide new insights for targeted therapy in CC. Overall, these findings highlight the potential and clinical utility of the SRL-based risk model and nomogram in predicting patient outcomes and guiding personalized treatment decisions in CC. To confirm the efficacy and applicability of this nomogram in clinical practice, further validation and prospective studies are needed.
While previous studies have explored modeling articles on SRLs in colorectal cancer, this current study offers several advantages over these works. Firstly, this study is the first to utilize the random forest method for modeling. The random forest method is known for its high accuracy and robustness, making it well-suited for developing prognostic models. By employing this method, the current study has achieved a higher level of accuracy in predicting patient outcomes. The selected signature in this study contains fewer genes compared to previous studies. This is significant because a smaller gene signature can streamline and simplify the prognostic model, making it more efficient and practical for clinical application.
Furthermore, the prognostic model developed in this study demonstrates a higher extrapolation value. It has been validated on two external datasets, which enhances the generalizability and reliability of the model. The validation process has resulted in a higher area under the curve (AUC) value, addressing the issue of insufficient extrapolation that may have been present in previous studies [44,45]. These advantages add to the significance and novelty of this study, culminating in a more accurate and reliable prognostic model based on SRLs in colorectal cancer. The utilization of the random forest method, the smaller gene signature, and the validation on external datasets all contribute to the robustness and applicability of this prognostic model.
In addition to the advantages mentioned earlier, our study also analyzed somatic mutation data, which was not previously done in research papers within this context. This analysis revealed significant differences in somatic gene mutations between the high- and low-risk groups of colorectal adenocarcinoma (COAD) patients. This novel aspect of our study provides valuable insights into the genomic landscape of CC and its association with the SRL-based risk model.
Furthermore, based on functional semantic similarity, our study utilized GO analysis and categorized the results into five groups. This approach provides a more comprehensive understanding of the potential biological processes associated with the SRLs. Finally, to further validate our findings, we selected the most significant lncRNA TSPEAR - AS2, and carried out phenotypic and animal experiments. This confirmed that inhibiting the expression of TSPEAR - AS2 can suppress the malignant phenotype of CC tumor cells. The identified categories and their correlation with CC provide valuable information for future research and serve as a foundation for further investigations in this field .
In conclusion, new avenues for the development of improved treatment strategies and clinical management for CC patients are opened up by the SRL-based risk model developed in this research. However, acknowledging certain limitations of the study is important. Firstly, despite the utilization of integrative bioinformatic methods, functional experiments are needed to further elucidate the biological processes influenced by the SRLs. Secondly, further definition and validation of the guidelines for implementing the SRL-based risk model in clinical settings is needed.
Despite these limitations, a significant contribution to the understanding of CC and a solid theoretical basis for further research and the development of personalized approaches in the management of this disease is provided by our study.
{kind=link}