A seventy-year-old man presented to the emergency department with worsening dyspnoea and lethargy over a three-week period following a confirmed COVID-19 infection on March 2022 with which he initially reported myalgias, cough and dyspnoea at rest. Of note, he had received three doses of the COVID-19 vaccine prior to this presentation. His subsequent COVID-19 PCR was negative at the time of this presentation. He currently denied fevers, chills and rigors nor any occupational or domestic exposures of note. His past medical history included hypertension and depression.
His initial physical examination revealed hypoxia needing 1 L of supplemental oxygen via nasal prongs to maintain saturations of 94% and above with a respiratory rate of 28 breaths per minute. Otherwise, he was normotensive and afebrile. He had decreased breath sounds at both bases with coarse crepitations to the mid-zones bilaterally. The remainder of his examination was unremarkable; including cardiopulmonary and abdominal exams. His neurological examination was also normal; notably with normal power at presentation.
Initial investigations revealed neutrophilia with WCC 15.2×109/L (normal ~ 2.0–8.0×109/L) with an elevated C-reactive protein (CRP) measuring at 96mg/L (normal < 3mg/L) and erythrocyte sedimentation rate (ESR) at 41 (normal < 21mm/h). Liver function testing demonstrated elevated transaminases (ALT 281 U/L, normal 4–36 U/L; AST 268 U/L, normal 8–33 U/L) with normal ALP and GGT. A chest X-ray found patchy opacification in bilateral lung spaces particularly involving the right mid to lower-zones, suggestive of atypical bronchopneumonia [Figure 1A, 1B]. The patient was empirically treated for a post-COVID-19 pneumonia with intravenous antibiotics which included ceftriaxone 1g daily and azithromycin 500mg daily.
The patient had improved clinically following intravenous antibiotics before being transitioned to oral amoxicillin/clavulanate for a further three days. However he deteriorated two days later on oral antibiotics with a saturation of 86% on room air with a respiratory rate of 30 breaths per minute. A CT chest was performed subsequently.
The CT chest revealed changes suggestive of fibrotic lung disease, consistent with usual interstitial pneumonitis (UIP) pattern consistent with a drug reaction or connective tissue-related interstitial fibrosis [Figure 1C, 1D].
[Figure 1]: [1A] Chest X-ray demonstrating right middle to lower zone patchy heterogenous opacification. [1B] Repeat Chest X-ray demonstrating partially resolved changes in right lung with new ground glass opacity in the right lung in the subpleural location. [1C] CT-chest (axial view) demonstrating basal and lateral fibrotic changes consistent with a usual interstitial pneumonitis (UIP) pattern. [1D] CT-chest (coronal view) demonstrating basal and lateral fibrotic changes consistent with a usual interstitial pneumonitis (UIP) pattern.
Given the CT findings, auto-immune serology was sent. The extractable nuclear antigen (ENA), the anti-neutrophil cytoplasmic antibodies (ANCA), complement levels, the cyclic citrullinated peptide (CCP) antibodies and rheumatoid factor (RF) were all negative. Due to the deranged liver enzymes, other atypical causes of pneumonia were considered. Chlamydia pneumonia serology demonstrated a positive IgG and a negative IgM antibody consistent with a previous exposure, and mycoplasma serology wasnegative.
Despite two courses of broad-spectrum intravenous antibiotics, the patient had ongoing respiratory symptoms and had persistently elevated inflammatory markers.
After three weeks, the patient had a significant decline in function. He was notable to perform personal activities of daily living and was noted to have difficulty getting out of a chair as well as walking. As such, he was transferred to the rehabilitation unit for ongoing care. Whilst in rehabilitation, the patient reported new oropharyngeal dysphagia, particularly coughing and spluttering when eating solid food. This was confirmed on a barium swallow, which found oesophageal dysmotility and diffuse oesophageal spasm.
A diagnosis of atypical COVID pneumonia with long COVID was made.
The patient represented the following day after a fall with a long lie of approximately 14 hours. A physical examination noted no injuries however the patient was feeling lethargic and weak. He also demonstrated quite profound upper and lower limb weakness consistent with proximal myopathy. His cervical flexion power was also found to be weak.
Further investigations were performed; there was a mild neutrophilia (10.7x109/L; normal ~ 2.0–8.0×109/L), thrombocytosis (platelets 511x109/L, normal 150-450x109/L), persistently elevated C-reactive protein (52.4mg/L, normal < 3mg/L) and a significantly elevated creatinine kinase (CK) (4301 U/L, normal < 201 U/L).
A chest X-ray showed the right lung heterogenous opacification had partially resolved, however there are some new ground glass changes in the right subpleural space. There was also new development of patchy opacification in the left lower zone with background fibrotic changes in the lungs.
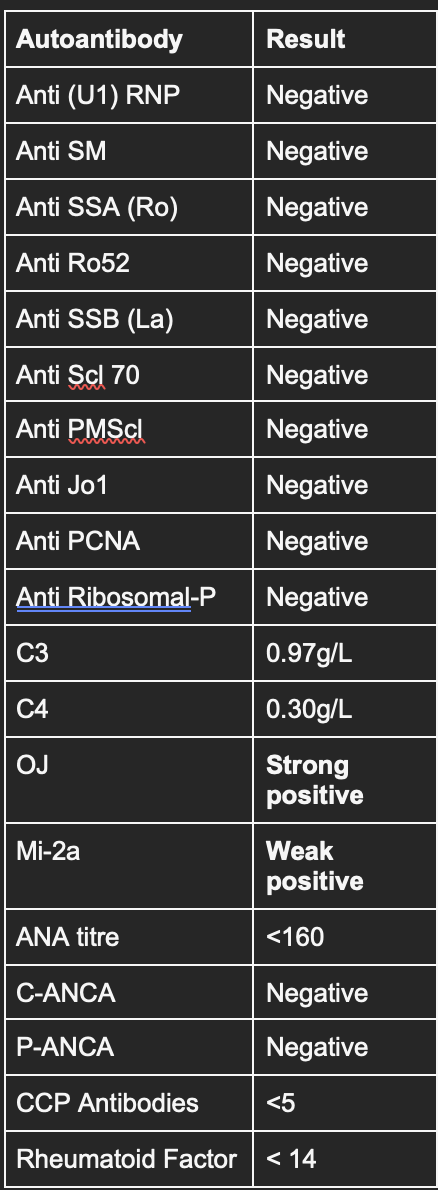
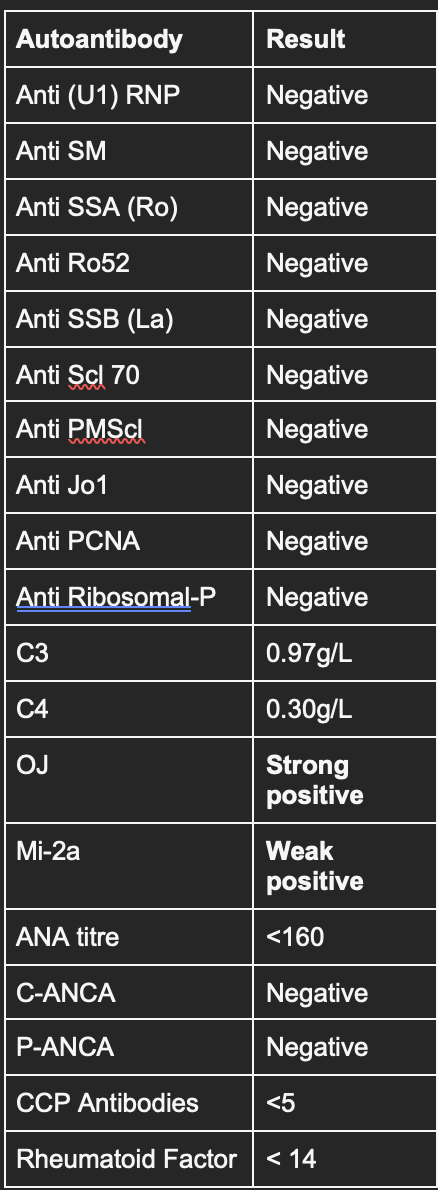
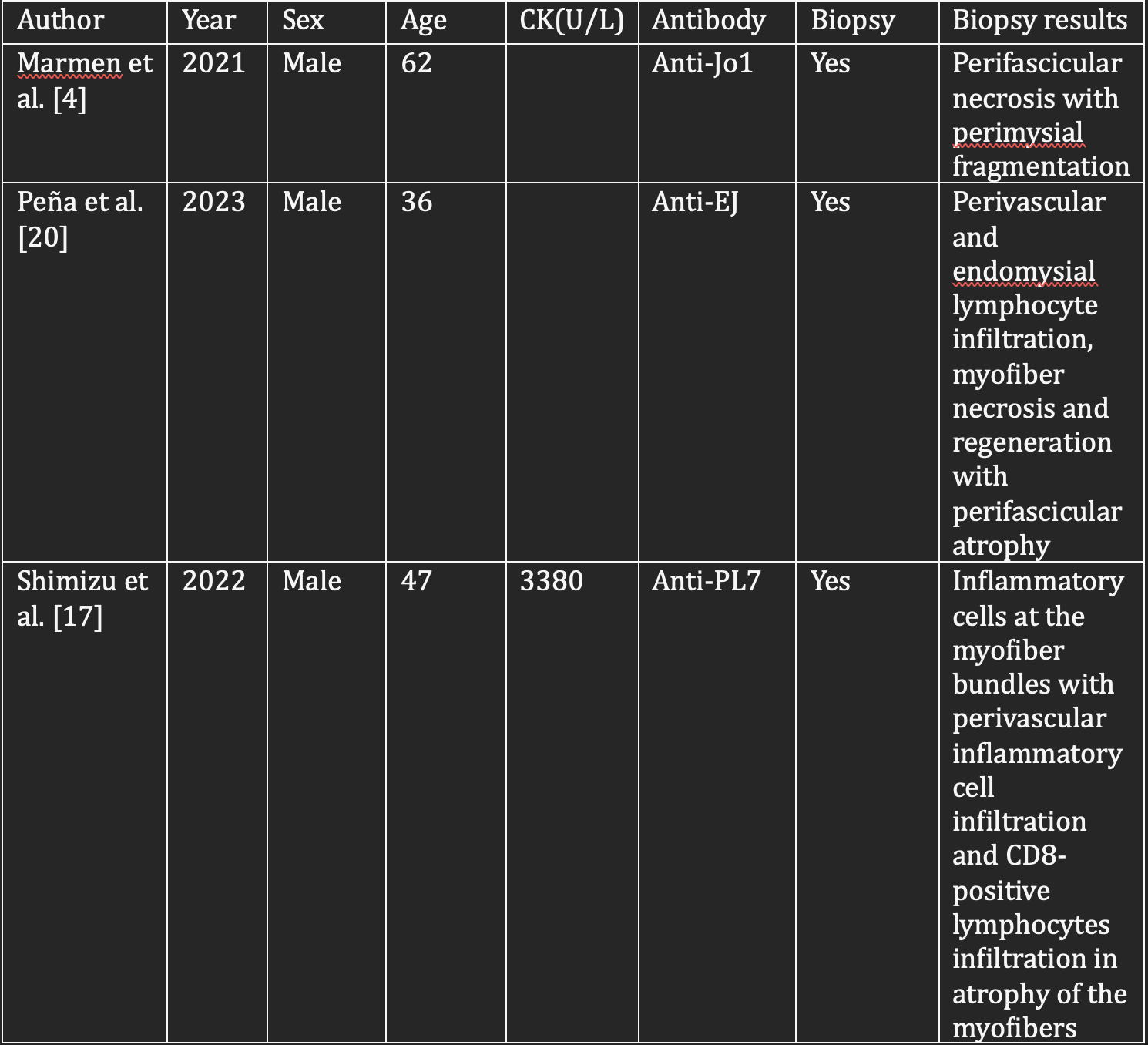
Due to the elevated CK, the dark-coloured urine and the fall with long lie, the patient was treated as rhabdomyolysis with fluid resuscitation. In spite of this, the patient’s CK remained elevated. Further testing revealed a strongly positive anti-OJ auto-antibody and a weakly positive Mi-2a auto-antibody [Table 1]. An MRI of his bilateral thighs were done [Figure 2A,2B] and subsequently a muscle biopsy was performed and showed numerous muscle fibres showing active degeneration with a tendency to perifascicular degeneration. There was no lymphocytic infiltration with a light histiocytic infiltrate in the perimysium and alkaline phosphatase was regulated in a perifascicular distribution [Figure 2C,2D]. A diagnosis was made of an active immune mediated perimysial muscle pathology (IMPP), in keeping with antisynthetase syndrome.
[Table 1]: Patient’s auto-antibody panel demonstrating positive anti-OJ auto-antibody.
[Figure 2]: [2A, 2B] MRI shows high signals on STIR bilateral thighs demonstrating mild diffuse myositis of the gluteal muscles and the muscles of the posterior thigh with mild generalised fatty atrophy. MRI, magnetic resonance imaging; STIR, short T1 inversion recovery. [2C] High power image of the skeletal muscle showing peri fascicular degeneration of muscle fibres x 400 actual magnification, Haematoxylin and Eosin. [2D] Low power image showing upregulation of alkaline phosphatase (black) in a peri fascicular pattern x 100 actual magnification, Alkaline phosphatase.
The patient received pulse methylprednisolone 1g for 3 days with a long oral prednisolone wean. In addition, he was then commenced and escalated to a full dose of azathioprine given a normal purine metabolism. In view of multiple end-organ manifestations, loading immunoglobulin at 2g/kg administered over two days was given. He was also given 1g/kg immunoglobulin at a four-weekly frequency as maintenance.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}