Maxillary permanent incisor torsion caused by supernumerary teeth is not frequently encountered in dental practice, but its treatment is challenging because of its importance for facial esthetics and the complexity of treatment. Timely intervention is often required to avoid severe complications. This article presents the case of a 7-year-old male patient with severe torsion of anterior teeth in mixed dentition. Multidisciplinary treatment was proposed to meet the patient’s needs, involving extracting the supernumerary teeth, using an intra-maxillary casting distractor and the 2×4 fixed orthodontic technique to align the severely twisted anterior teeth, and employing a Hawley retainer during the day and a customized silicone guide at night to maintain and guide occlusal development. At the end of treatment, the patient attained molar and canine class I with normal overjet and overbite. The combination of an intra-maxillary casting distractor and the 2×4 fixed orthodontic technique is very effective for treating severe torsion of upper anterior teeth if the patient is cooperative with using a retainer to prevent recurrence.
Case Report
Multidisciplinary treatment for severe torsion of anterior teeth : a case report
https://doi.org/10.21203/rs.3.rs-4218749/v1
This work is licensed under a CC BY 4.0 License
Version 1
posted
You are reading this latest preprint version
supernumerary teeth
anterior tooth torsion
mixed dentition
intra-maxillary casting distractor
customized silicone guide
Hyperdontia is an anomaly of an increased number of teeth. Supernumerary teeth can occur in both permanent and primary dentitions with an incidence ranging from 0.45–2%1, but are more frequently observed in the permanent dentition2. Males are twice more likely to have supernumerary teeth than females3. Mesiodens are the most frequent type of supernumerary teeth. They occur unilaterally or bilaterally in the maxillary anterior area4. Supernumerary teeth may be normally shaped or differ in appearance. They are often hypoplastic and can be positioned inside or outside the dentition. The appearance of supernumerary teeth can interfere with the eruption and normal development of other teeth, cause occlusal trauma, create new retention sites for food, and make it difficult to maintain adequate oral hygiene5, endangering periodontal tissue health4, 6, 7. Cystic formations can often develop around unexplained excess teeth5, 8. Significantly, supernumerary teeth can lead to severe torsion of anterior teeth in children in mixed dentition, affecting their physical and mental health, and require timely intervention.
Management strategies for children with impacted maxillary incisor teeth due to a supernumerary tooth generally involve a multidisciplinary approach9.For torsion of anterior teeth in children, the common treatment is the 2×4 fixed orthodontic technique. However, for children with severe torsion of anterior teeth in early mixed dentition, there are deficiencies in the number of tooth eruptions, the height of tooth eruptions, and the length of root development, meaning the 2×4 fixed orthodontic technique cannot directly correct severe torsion of anterior teeth. In addition, recurrence following treatment is a concern. Overcorrection, use of a retainer for a longer duration, early treatment, achievement of a good balance, and gingival circumcision can prevent recurrence10. However, stability after these treatments is poor and must be maintained for a long time.
This article aimed to report multidisciplinary treatment for severe torsion of anterior teeth caused by supernumerary teeth in a child in mixed dentition and to provide new treatment ideas for this disorder.
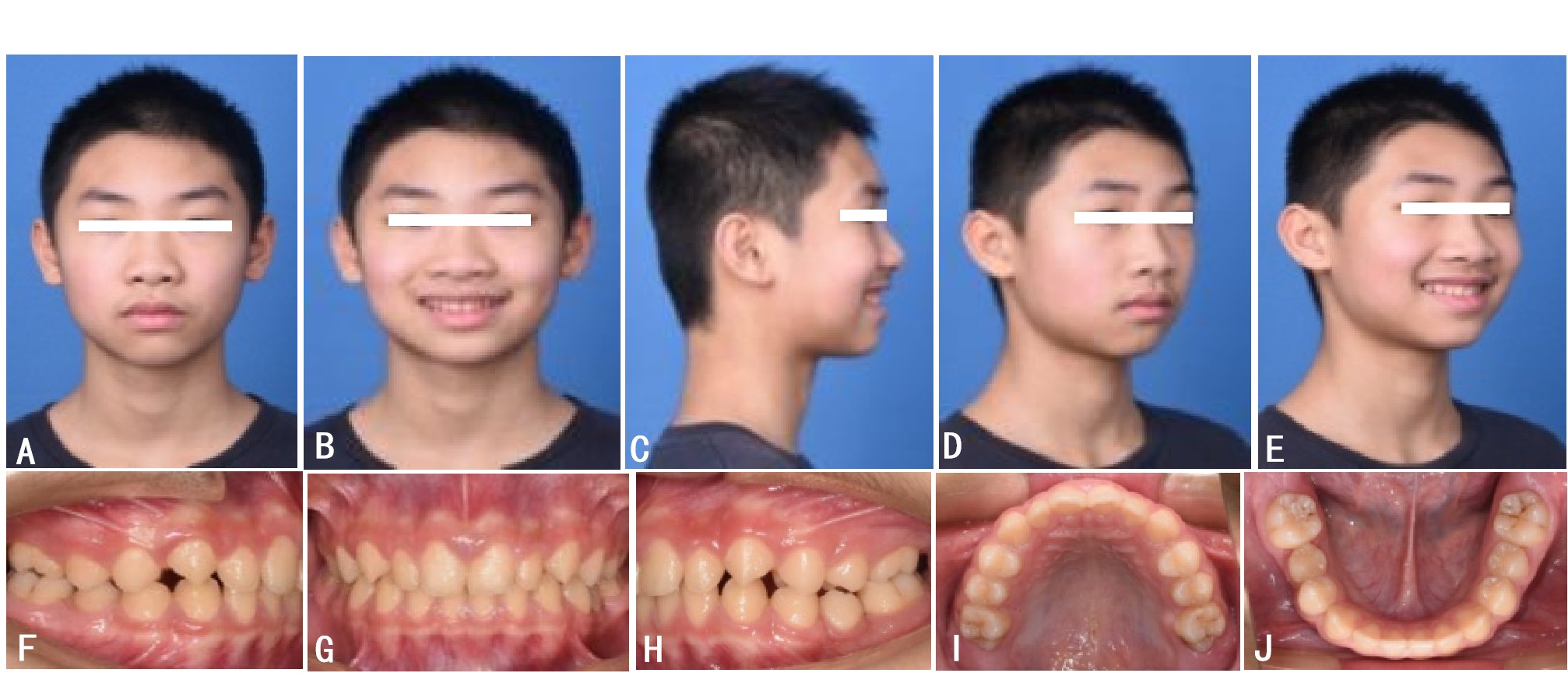
A 7-year-old boy had been mocked by his classmates for having irregular upper anterior teeth for half a year and sought medical attention. He had a history of mouth breathing for about 2 years. A thorough general examination was carried out to rule out the presence of any syndrome. Medical and family histories were non-contributory. Extra-oral examination revealed a convex soft tissue shape and mandibular hypoplasia (Fig. 1A–C). Intra-oral examination showed mixed dentition, which was normal for the boy’s age. In the anterior region of the maxilla, there was severe torsion of the anterior teeth (Fig. 1D–H). Teeth 11 and 21 displayed mesial 90° rotation, with about a 10-mm gap between them; the upper central incisors were located in the interproximal space between the lower central incisors and lateral incisors at the central occlusion; there was visible plaque + +; 31, 32, 41, and 42 gums were congested; and 41 gums were slightly retracted.
Periapical radiographs, a panoramic X-ray, a lateral cephalogram, and cone-beam computed tomography (CBCT) were performed. On X-ray, teeth 11 and 21 displayed about mesial 90° rotation (Fig. 2). The right supernumerary tooth was horizontally impacted and the crown was located on the palatal side, about 2 mm from the alveolar ridge. The left supernumerary tooth was parallel to the long axis of tooth 21 and was erupted submucosally. The lateral cephalogram showed a sagittal class II skeletal malocclusion (∠ANB, 5.9°) with vertical growth type (S-Go/N-Me, 60.4 and ∠SN-MP, 41.6°) (Fig. 3 and Table 1).
|
Measurement |
Initial |
Post-treatment |
Normal |
Standard deviation |
|---|---|---|---|---|
|
SNA (°) |
74.6 |
74.8 |
83.0 |
4.0 |
|
SNB (°) |
68.6 |
69.9 |
80.0 |
4.0 |
|
ANB (°) |
5.9 |
4.9 |
3.0 |
2.0 |
|
FMA (FH-MP) (°) |
28.9 |
28.4 |
26.0 |
4.0 |
|
Y-axis (°) |
62.9 |
63.2 |
64.0 |
2.0 |
|
SN-MP (°) |
41.6 |
41.3 |
30.0 |
6.0 |
|
S-Go/N-Me |
60.4 |
59.9 |
64.0 |
2.0 |
|
U1-SN (°) |
99.1 |
92.0 |
106.0 |
6.0 |
|
U1-NA (°) |
24.5 |
17.2 |
23.0 |
5.0 |
|
U1-NA (mm) |
3.5 |
2.1 |
5.0 |
2.0 |
|
U1-L1 (°) |
120.1 |
128.4 |
124.0 |
8.0 |
|
FMIA (L1-FH) (°) |
51.9 |
53.5 |
55.0 |
2.0 |
|
L1-NB (°) |
29.5 |
29.5 |
30.0 |
6.0 |
|
L1-NB (mm) |
5.7 |
7.2 |
7.0 |
2.0 |
|
Z-angle |
54.7 |
56.8 |
77.0 |
5.0 |
|
FH-N’Pg’ |
81.0 |
83.0 |
85.0 |
3.0 |
|
N’-Sn-Pg’ |
159.4 |
159.3 |
168.0 |
4.0 |
The diagnosis of this patient was as follows: 1) Angle class II with severe rotation of the upper central incisors, 2) sagittal type II, 3) vertical osteofacial pattern, 4) mild crowding of the upper dentition, 5) soft tissue convex, 6) early stage of growth and development, 7) supernumerary teeth at the maxillary midline, 8) plaque gingivitis, and 9) 41 gingival recession (occlusal trauma). The following treatment plan was developed: 1) preoperative ear, nose, and throat (ENT) consultation to exclude the possibility of obstructive lesions in the nasal airway, 2) extraction of supernumerary teeth, 3) orthodontic alignment of maxillary dentition, 4) oral hygiene guidance, and 5) maintenance.
Before orthodontic treatment, the supernumerary teeth were extracted to create a space for the upper central incisors (Fig. S1). The ENT consultation found no abnormalities in the airway. The orthodontic treatment was sequential, starting with aligning the upper anterior teeth (Fig. 4A–E). An intra-maxillary casting distractor was designed, which was bonded to the lingual buckle on the twisted tooth and pulled with elastic wire traction using light force (< 60 g), rotationally moving the severely twisted tooth so that it became mildly-to-moderately twisted (Fig. 4F), and then using the transpalatal arch and maxillary 2×4 fixed orthodontic technique to align the maxillary incisors after 41 days (Fig. 4G). The initial arch wire was 0.012 thermal activation wire, which was replaced once every 2 months three consecutive times, followed by 0.014 thermal activation wire and 0.016 wire; for 2 years and 4 months after surgery, 12–22 "8" ligation was used (Fig. 4H–L), during this stage, mandibular without any treatment.
After aligning the upper anterior teeth, the next stage was to maintain and guide the establishment of normal occlusion. The child wore a Hawley retainer during the day, and a customized silicone guide, as well as lip patches to assist lip closure, at night (Fig. 5A–E). Five years after treatment, when the patient was 12 years old, a physiological occlusion was initially established, with a coordinated profile and no caries. The pulp vitality test of teeth 11 and 21 showed no abnormalities, the periodontal tissue was healthy, and the tooth class was improved. There was a positive anterior overjet, resolution of the anterior crossbite, and upper and lower alignment, but still a slightly distal relationship of the first permanent molar and II° deep overbite (Fig. S2A–J). Therefore, the patient continued to wear the customized silicone guide at night for a year, combined with strong chewing function. At the end of the maintenance phase, a physiological occlusion was established (Fig. 5F-O), with a molar and canine class I relationship, normal overjet and overbite, midline alignment, and no temporomandibular joint-related symptoms. From a cephalometric point of view (Fig. 6B and Table 1), the inclination of the upper incisors and mandibular retraction were improved, which resulted in esthetic and functional enhancement. Pre-post cephalometric evaluation is provided in Table 1 and cephalometric tracing superimposition is shown in Fig. 6C-D.
Torsion of anterior teeth in mixed dentition affects oral function and facial esthetics in children, as well as physical and mental health. The larger the torsion angle, the more difficult it is to correct and the more serious the harm. When twisted central incisors lead to occlusal interference, there is not only occlusal trauma to individual teeth, which endangers periodontal tissue health, but also deviation or limitation of mandibular movement, as well as muscle dysfunction in closed mouth muscle groups, which causes temporomandibular joint disease. Therefore, it is necessary to select appropriate techniques for early correction.
The causes of tooth torsion are complex. Common causes are crowding; some congenital malformations and dental dysplasia, such as obstruction of supernumerary teeth to adjacent teeth, teeth around alveolar fissures, and teeth adjacent to congenital edentulous areas; local disorders in the mixed dentition period, such as heterotopia of permanent tooth germs, the impact of deciduous trauma on permanent tooth germs, and the effect of premature loss or retention of deciduous teeth on inherited permanent teeth; and other factors such as genetic and iatrogenic factors. In this case, two supernumerary teeth caused severe torsion of the anterior teeth.
For torsion of anterior teeth in children, the common treatment is the 2×4 fixed orthodontic technique. However, this technique could not be directly applied in this patient with severe torsion of anterior teeth in early mixed dentition. Removable appliances can be used to solve this problem. The principle is to use a pair of effective torsional couples in opposite directions to create a counter-rotational corrective force. In this case, based on the principle of force couples, an intra-maxillary distractor casted for the maxillary was designed, which was bonded to the lingual buckle on the twisted tooth and pulled with elastic wire traction using light force, rotationally moving the severely twisted tooth so that it became mildly-to-moderately twisted, and then the 2×4 fixed orthodontic technique was used to align the maxillary incisors.
Recurrence following treatment of twisted anterior teeth is a concern. In this case, we used a retainer for a prolonged duration, and the patient wore a Hawley retainer during the day and a customized silicone guide at night. In addition, lip sticking was used instead of gingival circumcision because when rotating and twisting the anterior teeth, although the periodontal ligament fibers were pulled, the periodontal soft tissues required a long period of adaptive remodeling. The fibrous tissue and roots in periodontal ligaments in early mixed teeth are developing and forming, and periodontal tissues respond well to orthodontic force and can eventually move and fix the teeth in a new position. Therefore, early blocking correction of twisted anterior teeth can have double the effect with half the effort.
In this case, in addition to severe torsion of teeth 11 and 21, there was skeletal class II malocclusion, mainly caused by long-term mouth breathing resulting in soft and hard tissue changes in the maxillofacial region. Traditional appliances that interfere with mouth breathing are precourt and lip shields. Lip sticking was applied to disrupt the habitual mouth breathing, while perioral muscle function was trained using a customized silicone guide to achieve the balance between occlusal and perioral neuromuscular function and to guide occlusal development, as reported previously11.
Children are in the active stage of growth and development, and craniomaxillofacial bones and dental occlusion dynamically change. Malocclusion is an irregular relationship between the teeth, dental arches, jaws, and craniofacial regions, and is mostly caused by developmental malformations. Over many years of clinical practice, we have closely combined pediatric stomatology with orthodontics and proposed a new idea of occlusal induction from the perspective of oral preventive medicine, called physiological oriented occlusal induction (referred to as iGo, symbolized as  ), a process of ceaseless regular observation during craniomaxillofacial growth and development in children12. In this case, physiologically oriented diagnosis and treatment for occlusal induction/oral health management were performed. Supernumerary teeth were successively extracted, a maxillary fixed technique was used to align the incisors, a Hawley retainer was used to maintain them during the day, and a customized silicone eruption guide was used to regularize the dental arch, disrupt mouth breathing, and guide construction at night, combined with strong masticatory function. After 6 years of oral health management, intervention, and guidance, a physiological occlusion was established and occlusal stability and esthetic improvement were achieved. The long-term stability of severely rotated upper incisors after orthodontic treatment requires further observation.
), a process of ceaseless regular observation during craniomaxillofacial growth and development in children12. In this case, physiologically oriented diagnosis and treatment for occlusal induction/oral health management were performed. Supernumerary teeth were successively extracted, a maxillary fixed technique was used to align the incisors, a Hawley retainer was used to maintain them during the day, and a customized silicone eruption guide was used to regularize the dental arch, disrupt mouth breathing, and guide construction at night, combined with strong masticatory function. After 6 years of oral health management, intervention, and guidance, a physiological occlusion was established and occlusal stability and esthetic improvement were achieved. The long-term stability of severely rotated upper incisors after orthodontic treatment requires further observation.
In this case, the patient had a strong desire to align his upper anterior teeth, and his excellent compliance allowed good results to be achieved without damaging the periodontium. If a patient is very cooperative in using a retainer to prevent recurrence, the combination of an intra-maxillary casting distractor and the 2×4 fixed orthodontic technique is very effective for treating severely twisted upper anterior teeth.
DATA AVAILABILITY STATEMENT
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
ETHICS STATEMENT
The studies involving human participant were reviewed and approved by the Ethical Committee of College of Stomatology, Hospital of Stomatology, Guangxi Medical University. The patient’s guardian provided their written informed consent to participate in this study.
- Buenviaje TM, Rapp R. Dental anomalies in children: a clinical and radiographic survey. ASDC J Dent Child 1984;51(1):42-6. PMID:6583219.
- Moraes RS, Farinhas JA, Gleiser R, Primo LG. Delayed eruption of maxillary permanent central incisors as a consequence of mesiodens: a surgical re-treatment approach. J CLIN PEDIATR DENT 2004;28(3):195-8. https://doi.org/10.17796/jcpd.28.3.e137l87242t86222.
- Alsani A, Balhaddad AA. Delayed Eruption of Maxillary Central Incisors Associated with the Presence of Supernumerary Teeth: A Case Report with 18 Months Follow-up. J Contemp Dent Pract 2018;19(12):1434-6. PMID:30713169.
- Shih WY, Hsieh CY, Tsai TP. Clinical evaluation of the timing of mesiodens removal. J CHIN MED ASSOC 2016;79(6):345-50. https://doi.org/10.1016/j.jcma.2015.10.013.
- Ata-Ali F, Ata-Ali J, Penarrocha-Oltra D, Penarrocha-Diago M. Prevalence, etiology, diagnosis, treatment and complications of supernumerary teeth. J Clin Exp Dent 2014;6(4):e414-8. https://doi.org/10.4317/jced.51499
- Ahammed H, Seema T, Deepak C, Ashish J. Surgical Management of Impacted Supernumerary Tooth: A Case Series. Int J Clin Pediatr Dent 2021;14(5):726-9. https://doi.org/10.5005/jp-journals-10005-2008.
- Barham M, Okada S, Hisatomi M, et al.. Influence of mesiodens on adjacent teeth and the timing of its safe removal. Imaging Sci Dent 2022;52(1):67-74. https://doi.org/10.5624/isd.20210218.
- Lee JY. Dentigerous Cyst Associated With a Supernumerary Tooth. Ear Nose Throat J 2020;99(1):32-3.14. https://doi.org/10.1177/0145561318823638.
- Seehra J, Mortaja K, Wazwaz F, Papageorgiou SN, Newton JT, Cobourne MT. Interventions to facilitate the successful eruption of impacted maxillary incisor teeth due to the presence of a supernumerary: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop 2023;163(5):594-608. https://doi.org/10.1016/j.ajodo.2023.01.004.
- Al-Jasser R, Al-Subaie M, Al-Jasser N, Al-Rasheed A. Rotational relapse of anterior teeth following orthodontic treatment and circumferential supracrestal fiberotomy. Saudi Dent J 2020;32(6):293-9. https://doi.org/10.1016/j.sdentj.2019.10.003.
- Lyu L, Zhao Z, Tang Q, Zhao J, Huang H. Skeletal class II malocclusion caused by mouth breathing in a pediatric patient undergoing treatment by interceptive guidance of occlusion. J INT MED RES 2021;49(6):3000605211021037. https://doi.org/10.1177/03000605211021037.
- Lyu L, Lin H, Huang H. The effect of combined maxillary pad movable appliance and FR-III functional appliance in the treatment of skeletal Class III malocclusion of deciduous teeth. BMC ORAL HEALTH 2022;22(1):485. https://doi.org/10.1186/s12903-022-02547-x.
The authors declare no competing interests.
- Fig.S1.jpg
Surgical extraction of supernumerary teeth under sedation and analgesia, and a periapical radiograph 2 weeks later.
- Fig.S2.jpg
Extra- and intra-oral photographs of the patient of the patient at 5 years after treatment. Frontal view and smile (A, B), right profile (C), 45° profile and smile (D, E), right lateral occlusion (F), frontal occlusion (G), left lateral occlusion (H), upper arch (I), and lower arch (J).
{kind=link}
{kind=link}