A case of a 60-year-old man (body weight of 100 kilograms) is presented. He is known with hypertension, active smoking, and heart failure with reduced left ventricular ejection fraction at 30% requiring cardiac resynchronization therapy with defibrillator implantation (CRT-D) - Saint Jude Medical as a primary prevention and coronary artery disease (a chronic occlusion of the ostium of a small diameter obtuse marginal artery requiring medical treatment and percutaneous angioplasty of the right coronary artery).
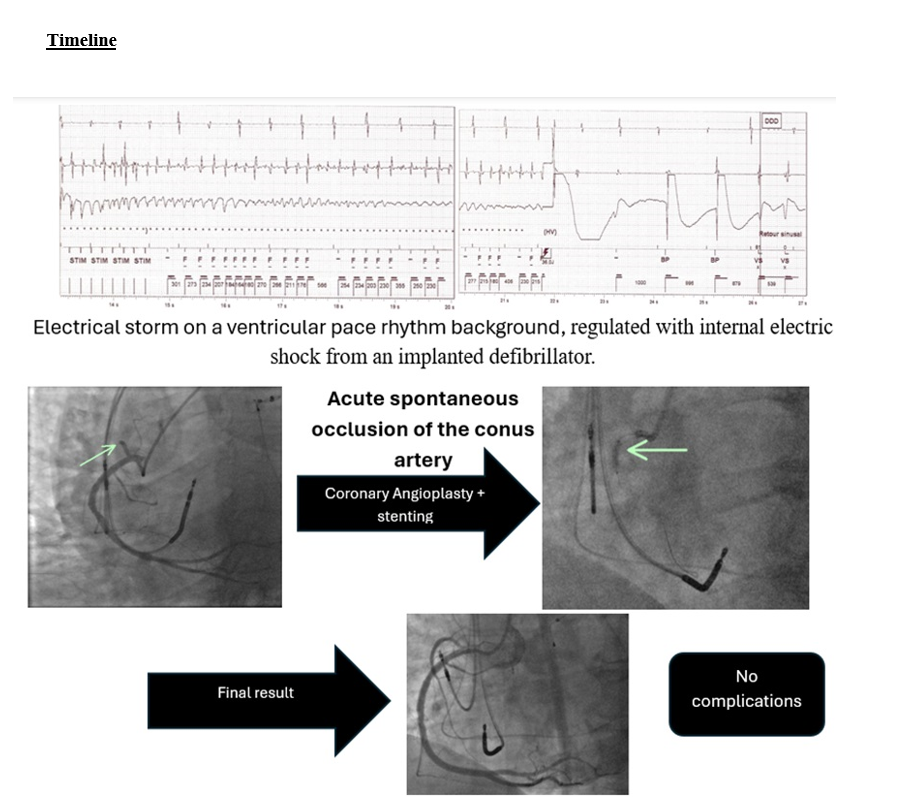
He presented to the emergency department after receiving multiple internal electric shocks delivered by his CRT-D over a 15-minute period, concomitant with a persistent oppressive chest pain. Vital parameters were within normal range, as well as physical examination. The initial electrocardiogram (EKG) showed a ventricular paced rhythm, like the patient's baseline EKG (Fig. 1).
The patient was treated with 300mg intravenous Amiodarone (Cordarone, Sanofi Winthrop industry, France) infused over 30 minutes. An interrogation of his CRT-D showed 13 episodes of ventricular fibrillation, each terminated by an internal electric shock (Figs. 2 and 3).
An emergency coronary angiogram was then performed, showing a known chronic occlusion of the second marginal, an absence of intrastent restenosis of the right coronary artery and an acute occlusion of the middle portion of the conus artery arising from the proximal segment of the right coronary artery persisting despite injection of 1mg intracoronary of Isosorbide Dinitrate (Risordan, Sanofi, France) (Fig. 4). The patient was treated with 250mg intravenous Acetylsalicylic Acid (Aspégic, Opella Healthcare France SAS, France), 180mg orodispersible Ticagrelor (Brilique; AstraZeneca, London, United Kingdom) and 50mg subcutaneous + 50mg intravenous Enoxaparin (Lovenox, Sanofi Winthrop industry, France).
A decision was taken to recanalize the occluded conus artery (culprit artery). The ostium of the right coronary artery was engaged with 6 French Amplatz® Left 0.75 (AL 0.75, 100 cm) Launcher guiding catheter (Medtronic Inc., Minneapolis, MN, USA). A 0.014" J-tipped Sion® Blue guidewire (Asahi Intecc Co. Ltd.) was inserted distally to the right coronary artery to improve support for the guiding catheter. The conus artery was recanalized with another 014" J-tipped Sion® Blue guidewire (Asahi Intecc Co. Ltd.), with recovery of a Thrombolysis In Myocardial Infarction (TIMI) Flow II.
A semi-compliant percutaneous coronary balloon angioplasty Ryurei® 2.0x15 mm (Terumo, Tokyo, Japan) was inflated at a maximum pressure of 12 atmospheres for a total duration of 15 seconds at the level of the occlusion, with a slow flow in the conus artery. The procedure was completed with the placement of a drug-eluted stent Orsiro® Mission 2.25x18 mm (Biotronik, Berlin, Germany) inflated at 14 atmospheres for a total duration of 20 seconds in the middle segment of the Conus artery. Final angiographic control showed a TIMI Flow III in the conus artery (Fig. 5) with complete recovery of the chest pain. No cardiac arrhythmias were noted during the procedure, during which the patient remained hemodynamically stable.
The patient was monitored in the cardiac intensive care unit. His post-intervention EKG remained unchanged. His blood analysis done prior to coronary angiography showed a slightly increased troponin level at 61 pg/ml (normal range < 34 pg/ml), normal creatine phosphokinases (CPK) at 199 IU/l (normal range 30–200 IU/l). The rest of the workup was unremarkable. The blood analysis performed 24 hours after the procedure showed a troponin peak above 50,000 pg/ml and CPK at 1,433 IU/l. Cardiac enzymes subsequently decreased. A cardiac ultrasound showed a known reduced left ventricular ejection fraction (32% calculated using the Simpson method), without pericardial effusion nor mechanical complications. The patient's clinical condition was stable during the hospital stay, without recurrence of chest pain nor arrhythmias.
{kind=link}