Participant recruitment
Patients who visited the neuropsychiatric department of our institute with a pre-existing mild cognitive impairment (MCI) or dementia diagnosis, individuals on their first visit for cognitive assessment, and individuals who responded to a hospital bulletin advertisement were enrolled. Patients who agreed to undergo both cognitive function testing and olfactory function testing between August 2018 and May 2019 were enrolled in this study. The inclusion criteria were (a) age > 50 years, and (b) being capable of complying with the study protocol. On the other hand, the exclusion criteria were as follows: (a) any past or current diagnosis of brain tumor, epilepsy, PD, major depressive disorder, bipolar disorder, or schizophrenia disease; (b) history of head trauma or stroke; (c) diagnosis of allergic rhinitis, acute/chronic rhinosinusitis, or a history of nasal surgery; (d) communication difficulties from severe hearing impairment or aphasia; and (e) failure to understand the study protocol and objectives. Information about the presence of the exclusion criteria was obtained through self-reporting by the enrolled subjects. Data on the demographic and clinical characteristics, including age, sex, smoking status, and diagnosis of AD or vascular dementia, were obtained from all the subjects. All experimental protocols were approved by the Institutional Review Board of the Chung-Ang University Hospital, and written informed consent was obtained from each participant and their caregiver (e.g., spouse or adult child).
Development of the sniffing bead system
The sniffing bead system was composed of several small beads (7 mm in diameter) and a handpiece (Additional file 1: Figure 1, Additional file 2: Video clip 1). The beads were designed such that any odor can be used. The beads containing the odorants are prepared beforehand, and the smell of the odorants can be maintained for more than six months if the beads are sealed. All the beads are only for a single-time use. In this study, we prepared beads packed with 2-phenylethyl alcohol (PEA), and beads with distilled water served as negative controls.
For the PEA beads, which have a rose-like smell widely used in olfactory testing [9], eight beads corresponding to eight different concentrations of PEA were used. PEA concentration was diluted in distilled water at a ratio of 1:2 (from 10–0.078%). The lowest concentration at which the subject detected the PEA odorant was scored as the PEA threshold score (scores: 1 [highest concentration] to 8 [lowest concentration], and 0 [not detected]).
To evaluate the generalizability of PEA sniffing bead system, n-butanol beads were prepared. For the n-butanol beads, which have an odor also commonly used for olfactory testing in the Korean population [8], eight beads corresponding to eight different concentrations of n-butanol were used. The n-butanol was diluted in distilled water at a ratio of 1:2 (from 4–0.0312%), with distilled water used as a negative control. The lowest concentration at which the subjects detected the n-butanol odorant was scored as the n-butanol threshold score (scores: 1 [highest concentration] to 8 [lowest concentration], and 0 [not detected]). The handpiece was composed of two parts: a plastic capsule and an aluminum body. The capsule could release the odor after bead insertion.
Olfactory threshold testing using the sniffing bead system
All olfactory function testing procedures were performed by two trained technicians in a well-ventilated laboratory lacking other scents, odors, or air currents. At the start of the test, the technician inserted only the bead containing distilled water into the handpiece and burst the bead 2 cm from the front of both nostrils. The patient was then asked if he/she recognized its odor. If the patient answered that he/she did not recognize any scent, the bead containing the fourth-strongest concentration (0.248% for PEA; 0.499% for n-butanol) was used. If the patient still did not recognize the scent, a higher concentration bead was used. Conversely, if the patient recognized the scent, a lower concentration bead was used. The lowest concentration at which the patient recognized the scent was recorded as the threshold for the PEA sniffing bead system. The time taken for each test was measured from the beginning to the end of the test by the technician.
YSK olfactory function testing
The YSK olfactory function test (RHICO Medical Co., Seoul, Korea) [10] is an olfactory testing instrument designed specifically with odors that are familiar to Koreans. It was used as the comparative standard olfactory function test in this study. The test battery included three subsets (i.e., threshold, discrimination, and identification tests). The test was performed in the same manner as the KVSS II [11]. In brief, the detection threshold was defined as the concentration at which the PEA (highest concentration: 10%, 1:2 serial dilutions to 12 steps) was correctly identified four times in a row. The test was performed using a triple-forced-choice paradigm and a seven-reversal initially ascending single-staircase procedure as described by Doty et al. [12]. For the discrimination test, triplets of odorants—two identical, one different—were presented, and subjects were asked to choose the odd, i.e., different odorant. Twelve pen triplets were presented to the subjects. The identification test involved a multiple forced choice from four descriptors. The sum of the three test scores was calculated as the threshold-discrimination-identification (TDI) score. The score of each test ranged from 1 to 12 for the threshold test, 0 to 12 for the discrimination test, and 0 to 12 for the identification test. The combined TDI score ranged from 1 to 36. Olfactory functions of the enrolled subjects were grouped as normosmia, hyposmia, and anosmia based on TDI score of the YSK test. The time taken for each test was measured from the beginning to the end of the test.
Neurocognitive testing
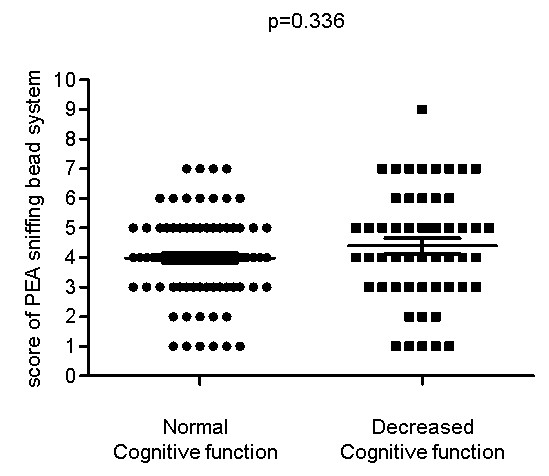
Two psychiatrists evaluated all the subjects for cognitive function and major neurocognitive disorders using the Structured Clinical Interview for DSM-5 Disorders—Clinician version (SCID-5-CV) [13]. The Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease-Korean version assessment packet (CERAD-K) [14] and the Korean version of the Mini-Mental State Examination [15] were also administered to all the subjects. The CERAD-K consists of the following items: Verbal Fluency, Modified Boston Naming, Mini-Mental State Examination, Word List Memory, Constructional Praxis, Word List Recall, Word List Recognition, Constructional Praxis Recall, Trail Making Test, and Stroop Test. We obtained each participant’s sub-scores, total score (from 0 to 100), and three cognitive function levels after adjusting for age and sex (normal range, significant decline but not dementia level, or impaired performance comparable to dementia). The subjects were divided into two groups based on the results of the CERAD-K examinations: subjects with normal cognitive function and those with impaired cognitive function [14,16].
Statistical analyses
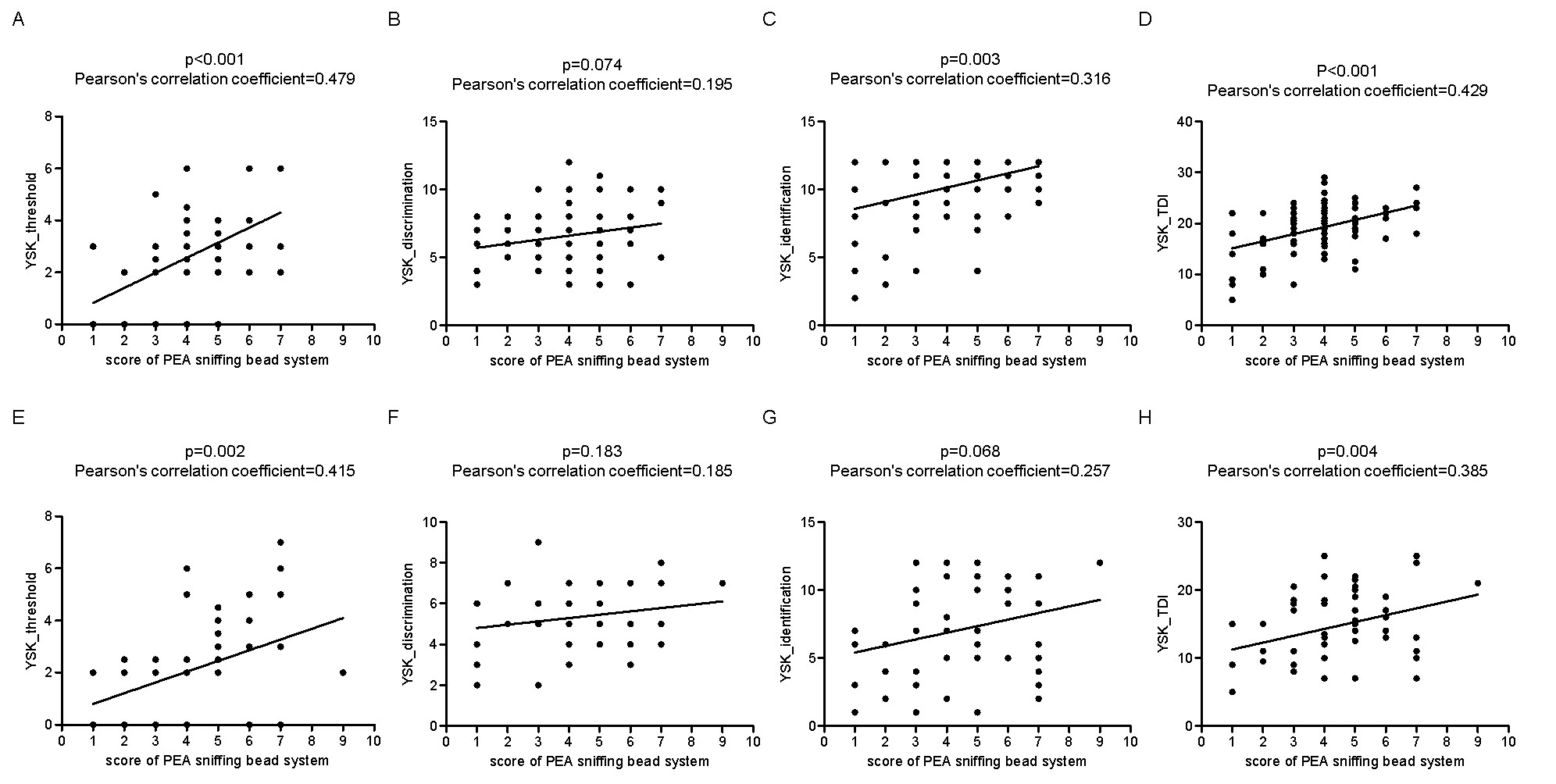
All the statistical analyses were performed using SPSS version 19.0 (IBM Corp., Armonk, NY, USA). Descriptive data were presented as means ± standard deviations and categorical data as frequencies (n) and percentages (%). The Pearson’s correlation coefficient was used to evaluate the association between two variables of interest. Differences between two groups were evaluated using the independent t-test. To test for differences among the three groups, a one-way Analysis of variance (ANOVA) was used with a Bonferroni post-hoc test. A p-value < 0.05 was considered statistically significant.
{kind=link}
{kind=link}
{kind=link}