Patient Selection
This subanalysis delves into the comprehensive dataset generated by the prospective trial titled "Accuracy of Myocardial Biomarkers in the Diagnosis of Myocardial Infarction After Revascularization as Assessed by Cardiac Resonance: The Medicine, Angioplasty, Surgery Study V (MASS-V)". Details on study design and protocol are published elsewhere (12). In summary, a total of 202 patients were enrolled, meeting the criteria of having multivessel coronary artery disease (CAD) with normal left ventricular ejection fraction (LVEF), and an indication for coronary artery bypass grafting (CABG) or percutaneous coronary intervention. Individuals with recent (<6 months) myocardial infarction, overt or suspected infections, active rheumatologic diseases, chronic renal failure (creatinine > 2.0 mg/dL), recent (<6 months) pulmonary embolism or venous thromboembolism, and contraindications to cardiac magnetic resonance (CMR) such as pacemaker implantation or severe claustrophobia were excluded from the study. All enrolled patients underwent CMR within six days of the revascularization procedure. The study was conducted in accordance with the principles outlined in the Helsinki Declaration and received approval from the institutional ethics committee at the Heart Institute of the University of São Paulo Medical School, São Paulo, Brazil. Informed consent was obtained from all participants. Out of the original 202 patients, a subset of 155 individuals qualified for this subanalysis, with 35 excluded due to incomplete T1 mapping phases acquisition and 12 experiencing CMR image artifacts hindering proper analysis.
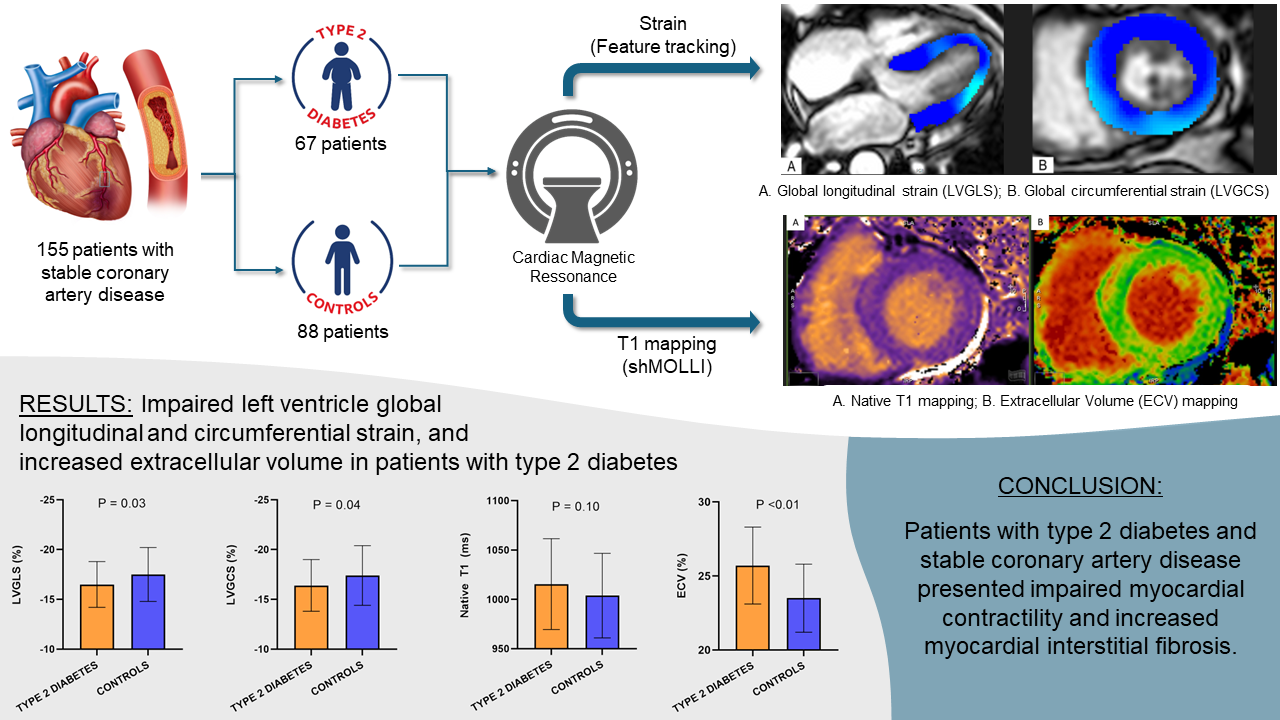
CMR, Strain, and T1 Mapping CMR examinations were conducted using a 1.5 Tesla Philips Achieva® scanner equipped with a dedicated 5-element phased-array cardiac surface coil, ensuring high-quality imaging. Electrocardiogram (ECG) synchronization was employed throughout the imaging process. Standard steady-state free precession (SSFP) cine sequences were acquired in both short and long axes of the left ventricle, capturing 30 cardiac phases to achieve sub-50 ms temporal resolution. Parameters such as left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), left ventricular ejection fraction (LVEF), and left ventricular mass (LVM) were measured and indexed to body surface area (BSA) (16). Late gadolinium enhancement (LGE) imaging was performed using phase-sensitive inversion recovery (PSIR) (15). CMR feature tracking (CMR-FT) was conducted using short-axis cine images and 2- and 4-chamber long-axis images. Manual delineation of end-diastolic left ventricular endocardial and epicardial contours in all images was followed by automated tracking, enabling the calculation of left ventricular global longitudinal strain (LVGLS), left ventricular global circumferential strain (LVGCS), and left ventricular global radial strain (LVGRS) (Figure 1). T1 mapping images were acquired utilizing the short modified Look-Locker inversion recovery (shMOLLI) technique in three short-axis slices (basal, middle, and apical). These images provided native T1, post-contrast T1, and extracellular volume (ECV) measurements (Figure 2) (13, 14). Native T1 was obtained before the administration of gadolinium-based contrast, while post-contrast T1 was acquired 15-20 minutes after intravenous injection of gadoterate meglumine (0.1 mmol/kg body weight). ECV was calculated using the formula: ECV = λ x (1-hematocrit [HT]). The partition coefficient (λ) was determined as λ = ΔR1myocardium/ΔR1blood, where ΔR1 represents the difference in relaxation rates (1/T1) before and after contrast administration. Notably, only segments without LGE were included in native T1, post-contrast T1, and ECV assessment. Trabeculae and papillary muscles were excluded from myocardial evaluation. All analyses were performed offline using dedicated commercial software (Cvi42) by two blinded observers. Discrepancies were resolved through consensus, or consultation with a third blinded observer if necessary.
Statistical Analysis
Continuous variables were described using means and standard deviations (SD) for normally distributed data or medians and interquartile ranges (IQR) for non-normal data. Categorical variables were presented as frequencies and percentages.
Comparisons between groups for categorical variables were performed using chi-squared tests, Fisher's exact tests, or likelihood ratio tests, depending on the number of expected cells per category. The Shapiro-Wilk test assessed normality of distribution for continuous variables. Normally distributed data were compared using Student's t-tests, while Mann-Whitney U tests were used for non-normal data. Univariate associations were evaluated with Pearson or Spearman correlation coefficients, depending on data normality.
Multivariate linear regression analysis explored the relationship between native T1, ECV, LVGLS, LVGCS, LVGRS, and the presence of T2D, additionally considering other relevant factors. Variables included in the model were clinically relevant or demonstrated statistical significance (p < 0.2 in univariate analysis).
All analyses were conducted using R software (version 3.6.2), with statistical significance set at p < 0.05.
{kind=link}