Neurocysticercosis is one of the most common neurological disorders and a public threat in many portions of the world (Butala et al., 2021). The condition arises due to the presence of cysts from Taenia solium in the brain and exhibits various clinical manifestations. The genetic background of the host and the inflammatory reaction of the host play a role in determining the severity of the disease (Ta and Blond 2022). Inflammatory responses in Neurocysticercosis vary depending on the location of the cysts. Once established within the Central Nervous System (CNS), the cysticercus triggers an immunomodulatory reaction, dampening the inflammatory response and facilitating the parasite's survival (Prodjinotho et al., 2020). However, when degeneration and death of the cysticercus occur, this immunomodulation is disturbed, provoking an inflammatory reaction linked to severe NCC symptoms like seizures and encephalitis.
Therefore, it is crucial to manage NCC treatment carefully to prevent adverse inflammatory outcomes in the CNS (WHO, 2021). Despite the widespread impact of NCC globally, many aspects of the disease remain uncertain. Many clinicians do not prescribe Anti Helminth Drugs (AHD) without brain imaging because of the great risk linked with the inflammatory response which varies with the location and number of the viable cysts present. The severity of the disease and its prognosis are closely correlated with both the intensity of the host's inflammatory response against the parasite and the localization of cysticerci (Fleury et al., 2004). Due to the significance of neuroinflammation in the development of NCC, extensive efforts have been made to understand and characterize the immune-inflammatory response in NCC and its role in combating the parasite
An AHD seems to be effective and in fact, a single cycle of treatment can make cysticerci calcified or disappear. But in the case of extra parenchymal NCC, when cysticerci present in the subarachnoid space of the base, the symptoms shown are diverse such as hydrocephalus, vasculitis, and arachnoiditis. In such cases, AHD treatment demonstrates limited effectiveness, with nearly one-third of patients requiring more than two cycles of treatment (Fleury et al., 2011). The reason behind this poor response to AHD is yet to be elucidated. As the simultaneous administration of the corticosteroid which helps to reduce severe inflammation might be involved. Corticosteroids, being immunosuppressive, reduce the host's specific immunity against the parasites. This specific immunity, in conjunction with AHD, is necessary to eradicate the parasite (Guilpain et al., 2012). All these observations drive us to investigate the relevance of differential responsiveness to cysticidal drug treatment accompanying the immune inflammatory profile.
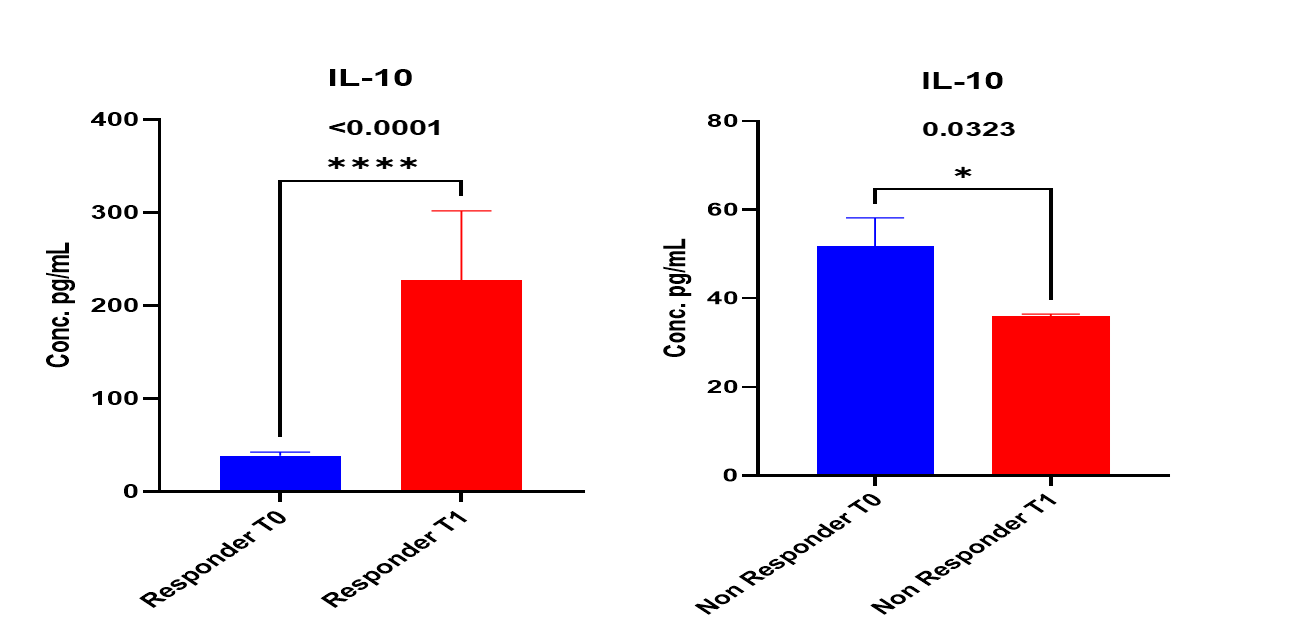
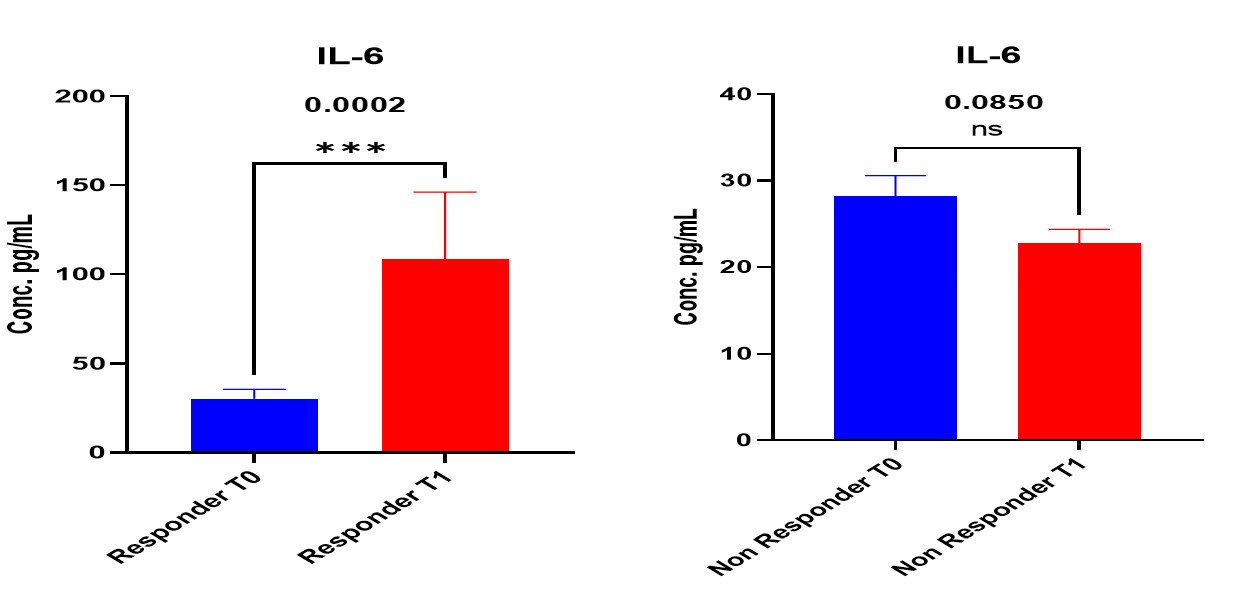
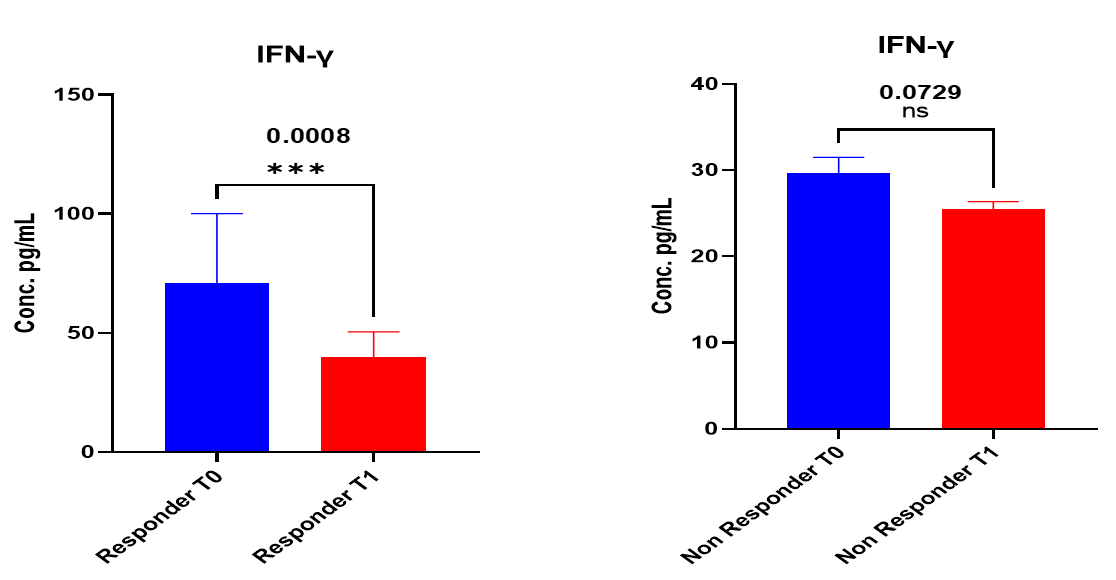
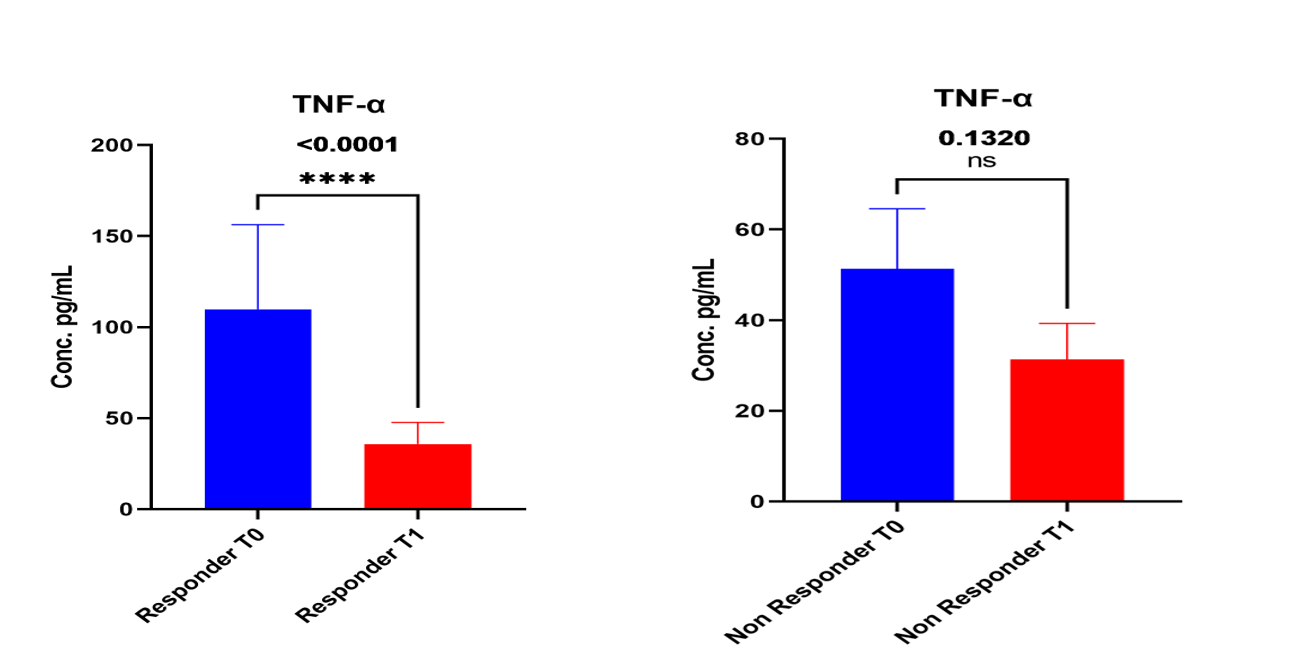
Variations are found in the immunological profile of various forms of NCC such as in the case of Parenchymal NCC in which the TH2 profile is dominant while in Extraparenchymal NCC depressed lymphocyte proliferative response is observed. The severity of Neurocysticercosis and its prognosis following AHD treatment are closely linked to peripheral and local inflammation. So, the objective of this study is to analyze the immune profile of patients before and after treatment, to assess the response of AHD concerning host immune response. This observation may imply a potential impact of cytokines on the efficacy of AHD treatment, as indicated by radiological findings.
It implies a possible role of the host's immune system in determining the efficacy of AHD treatment.
{kind=link}
{kind=link}
{kind=link}
{kind=link}