The present study marks a significant milestone as the initial inquiry revealing the complementary benefit associated with ICDs in reducing all-cause mortality. Notably, this effect was detected in patients with HFrEF who concurrently underwent quadruple GDMT, which included ARNIs, beta-blockers, MRAs, and SGLT-2 inhibitors. The findings of our study contribute to the ongoing discourse on the efficacy of ICD therapy in the context of contemporary HFrEF management. Our investigation focused on a cohort of patients adhering to the recommended quadruple GDMT comprising an ARNI, beta-blockers, MRAs, and SGLT-2 inhibitors. The literature extensively supports the individual and combined benefits of ARNIs, BBs, MRAs, and SGLT-2i in reducing mortality among HFrEF patients [1-11]. However, the role of ICD therapy in the era of contemporary medical therapy has been a subject of debate, with limited evidence on its effectiveness in conjunction with the latest therapeutic standards.
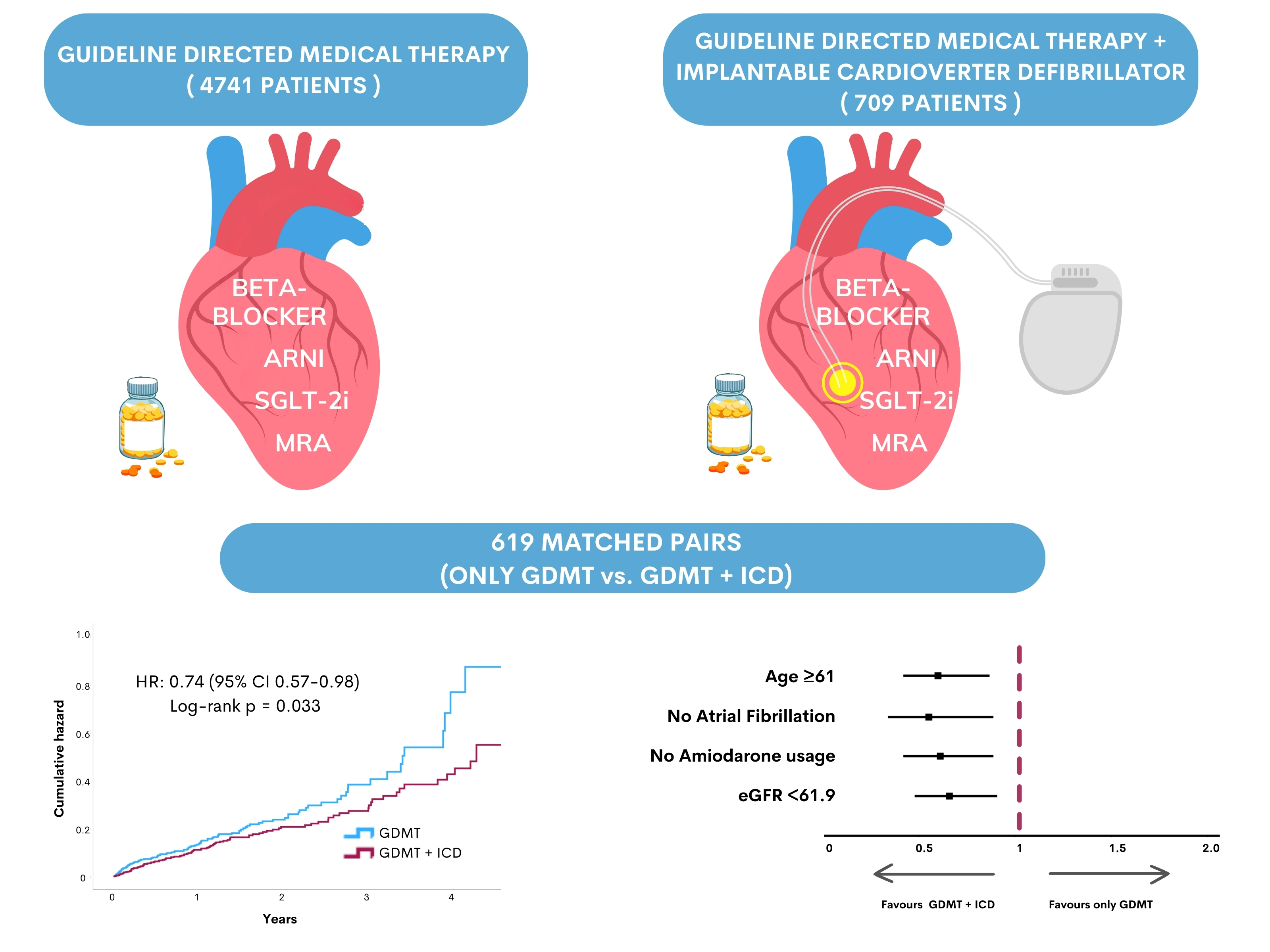
Our study revealed a noteworthy reduction in all-cause mortality associated with ICD therapy among HFrEF patients receiving quadruple GDMT. According to the matched cohort analysis, patients with ICDs had a 26% lower risk of all-cause mortality than those with only GDMT. These findings align with earlier landmark trials, such as the MADIT-II, which demonstrated the benefit of ICDs in reducing all-cause mortality in ischemic HFrEF patients [12]. Importantly, our study extends this observation to a contemporary cohort receiving the best optimal medical therapy, which includes ARNI, BB, MRA, and SGLT-2i.
The favorable impact of ICD therapy persisted across various subgroups, reinforcing its potential benefits in specific patient populations. Notably, older individuals (61 years and older), those without atrial fibrillation, individuals using amiodarone, and those with an estimated glomerular filtration rate (eGFR) less than 61.9 displayed a more pronounced reduction in all-cause mortality with ICD therapy. In our study, the addition of ICD therapy to the GDMT in patients with ischemic heart failure tended to reduce mortality, supporting the findings of the MADIT II study [12]. On the other hand, in patients with nonischemic etiology of HF, the addition of ICD therapy to GDMT did not improve all-cause mortality, consistent with the findings of the DANISH study [13].
The DEFINITE study examined the effect of ICDs on individuals with nonischemic dilated cardiomyopathy and revealed that those who received an ICD had a lower mortality rate during an average follow-up of 29 months [15]. However, the medical treatment for patients in this study primarily consisted of beta-blockers and ACE inhibitors. Moreover, the MUSTT study showed a survival benefit for patients with ischemic heart failure who took beta-blockers due to their antiarrhythmic effects [16]. However, contemporary heart failure management has shown that other medications also contribute to these effects. Since our study included patients with strong medical management, including ARNI and SGLT-2 inhibitors known for their anti-sudden death and anti-arrhythmic effects, we provide more up-to-date data on this topic.
The DINAMIT study examined the use of prophylactic ICD after acute myocardial infarction in the early period and found no significant difference in all-cause mortality between the groups [17]. Similarly, this study's background medical treatment primarily consisted of beta-blockers and ACE inhibitors. Our study included patients who received ICD implantation for both primary and secondary prophylaxis, and we observed that ICD implantation tended to be more beneficial for individuals with ischemic heart failure than GDMT. However, this trend did not reach statistical significance.
In our study, we found that the use of an ICD in addition to optimal medical therapy did not have a positive effect on all-cause mortality in patients who were using amiodarone. Amiodarone is a traditional medical treatment for preventing fatal arrhythmias in patients with a reduced ejection fraction, but its efficacy in heart failure patients has been inconsistent across various studies [18, 19]. The SCD-HeFT study showed that ICD usage was superior to amiodarone in patients with an LVEF <35% and New York Heart Association (NYHA) class 2-3 [20]. In our study, after propensity score matching, the rate of amiodarone use was similar in both groups. Previous studies have shown low utilization rates of optimal medical therapy, and the effectiveness of amiodarone in heart failure patients needs to be reevaluated. In our subgroup analysis, we found that ICD implantation significantly improved survival in patients with HFrEF who did not receive amiodarone. Therefore, in patients receiving GDMT, especially if amiodarone usage is restrictive, ICD implantation is considered a significant opportunity for improving survival.
Limitations
While our findings suggest a continued benefit of ICD therapy in the contemporary era of HFrEF management, it is essential to acknowledge the limitations of our study. The retrospective nature of the investigation and the reliance on deidentified data introduce inherent biases. Additionally, the absence of data on certain variables, such as cause-specific mortality and device programming details, limits the depth of our analysis. The patients included in the study are those with HFrEF due to the requirement of medical indication, but the lack of available average LVEF values is another limitation of the study.
{kind=link}