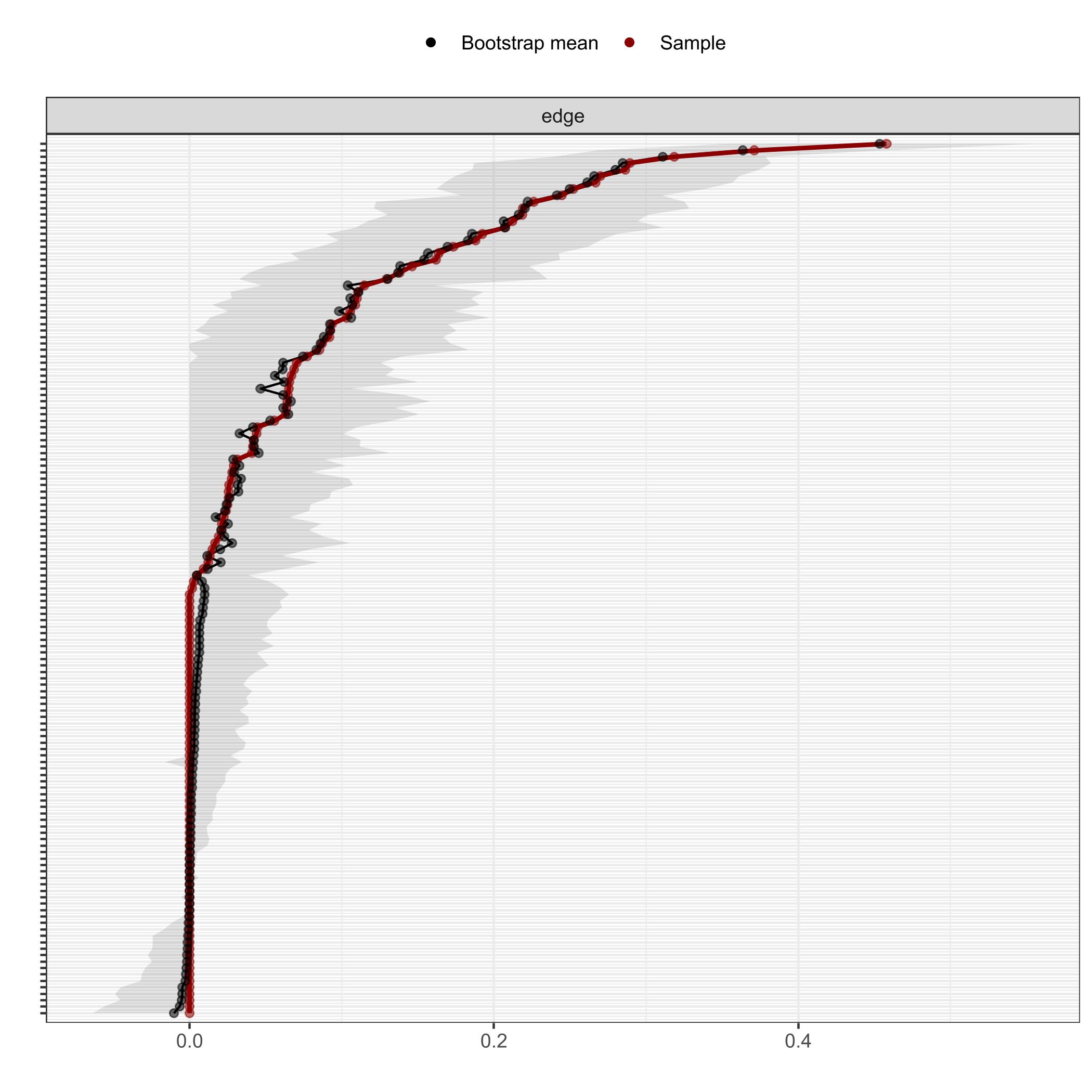
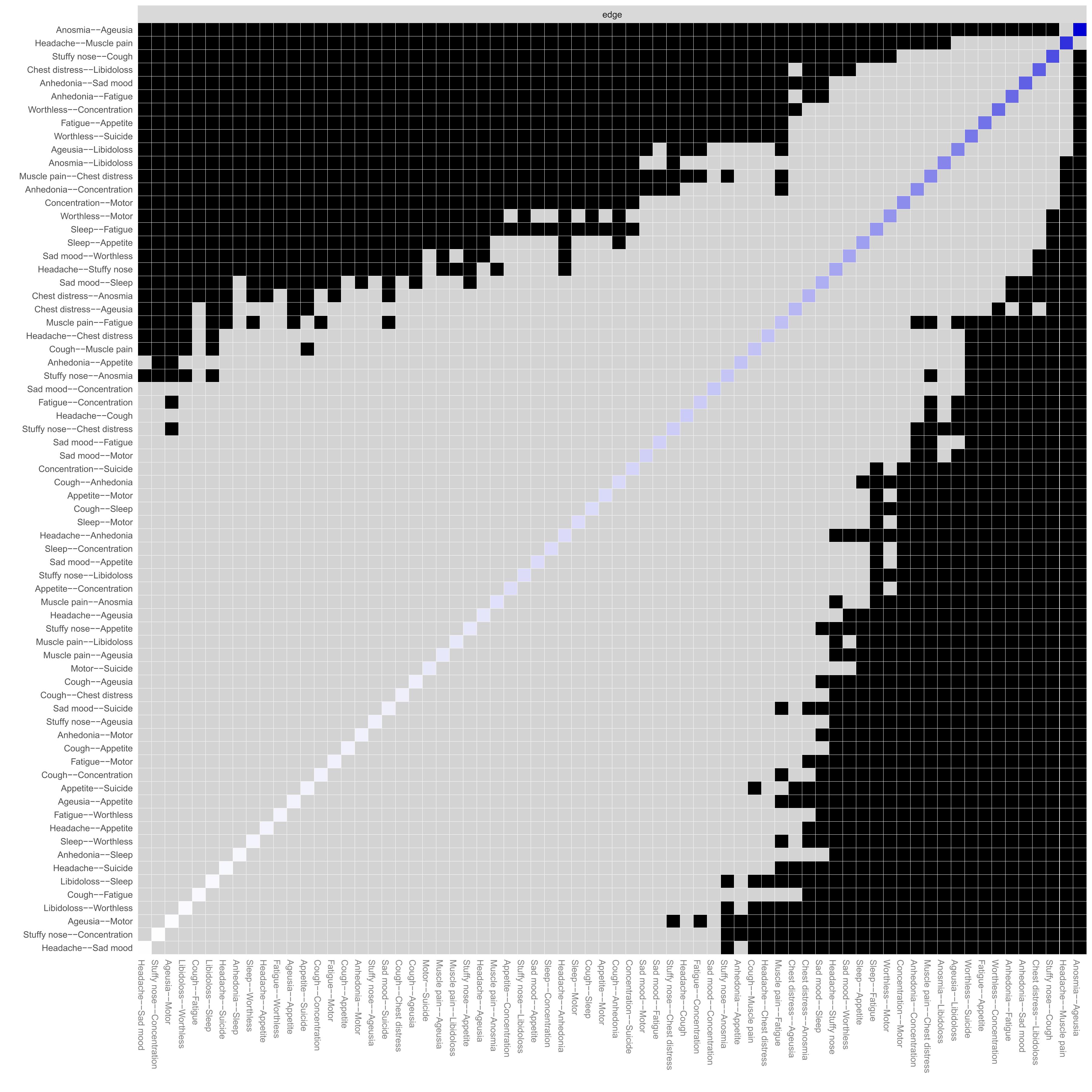
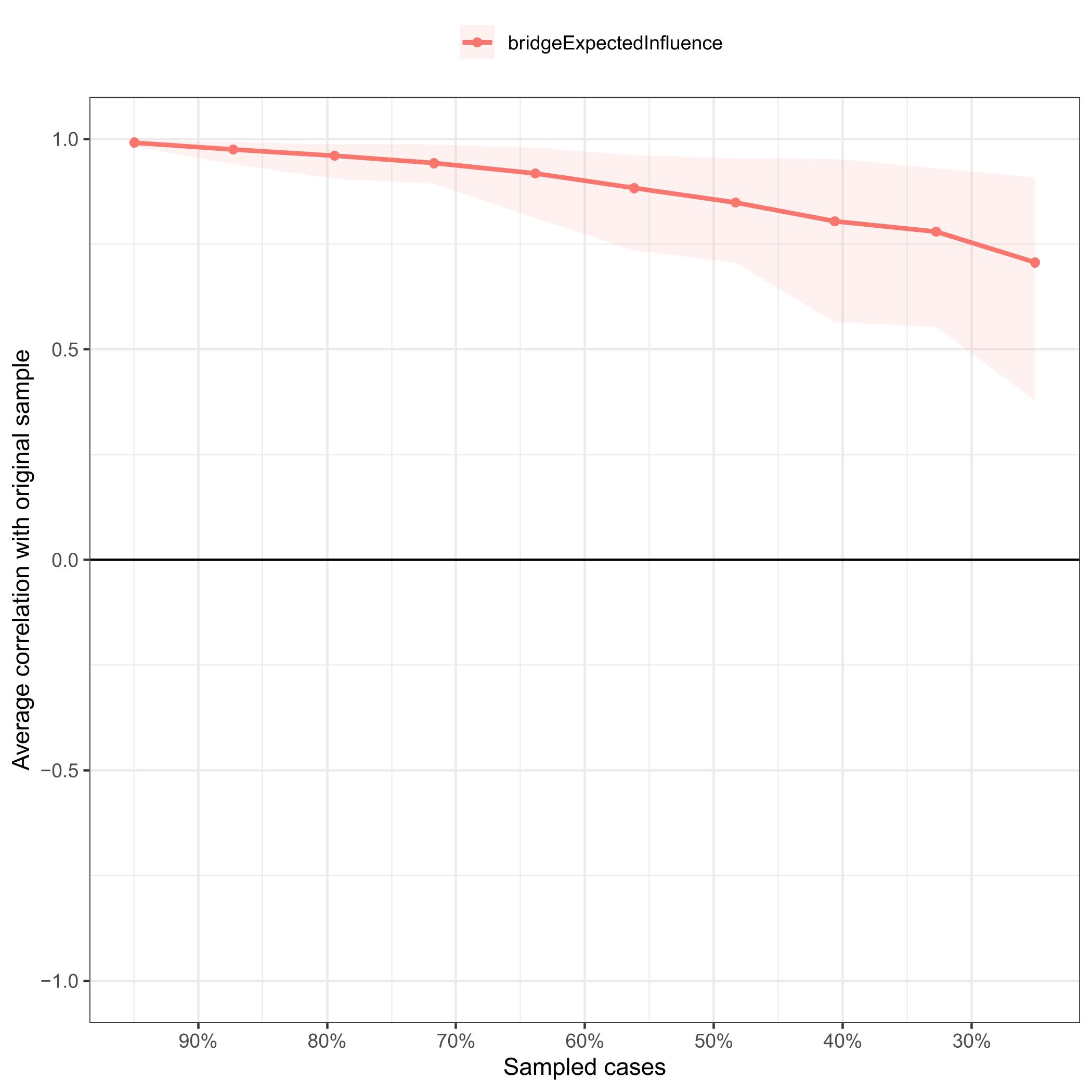
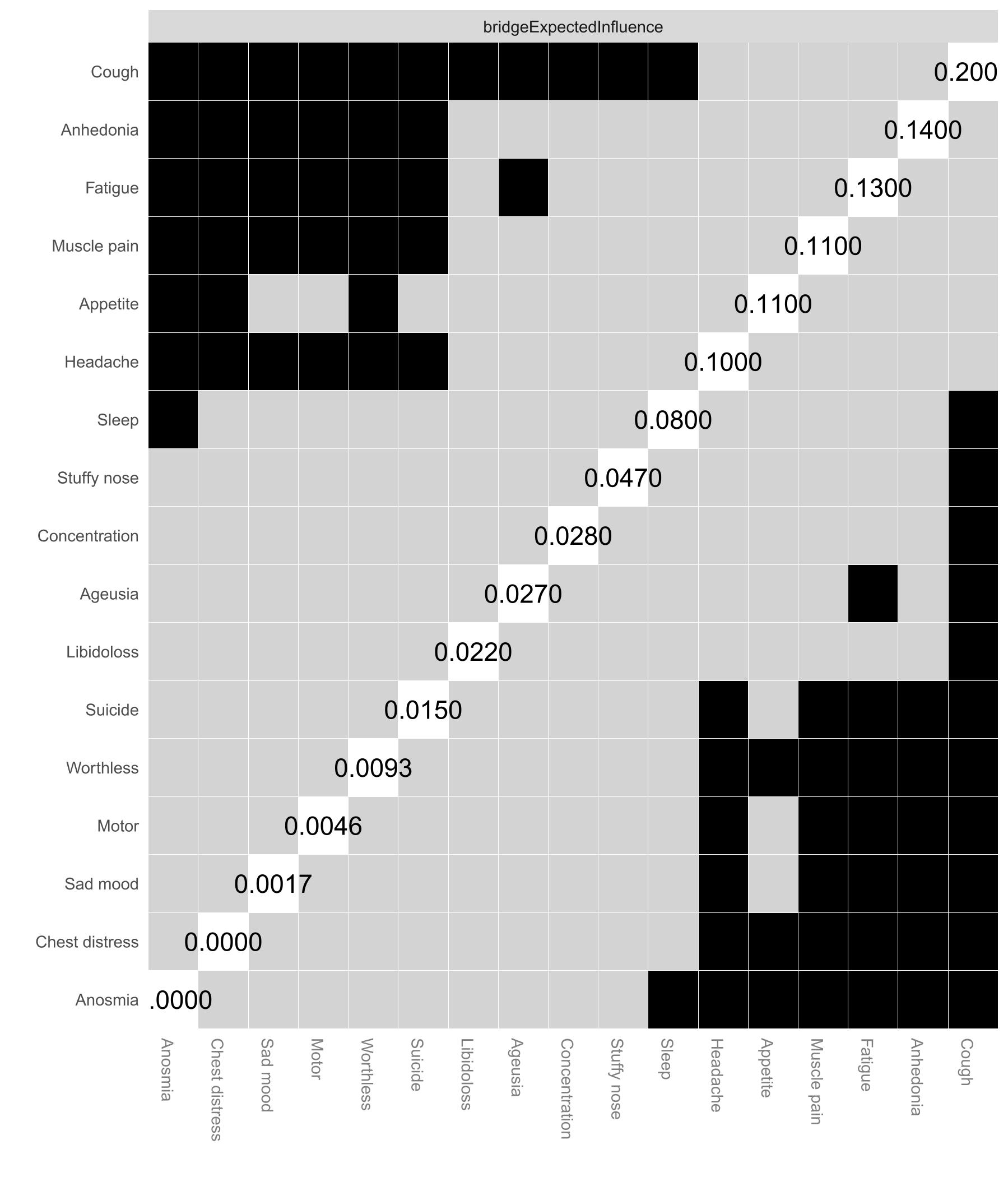
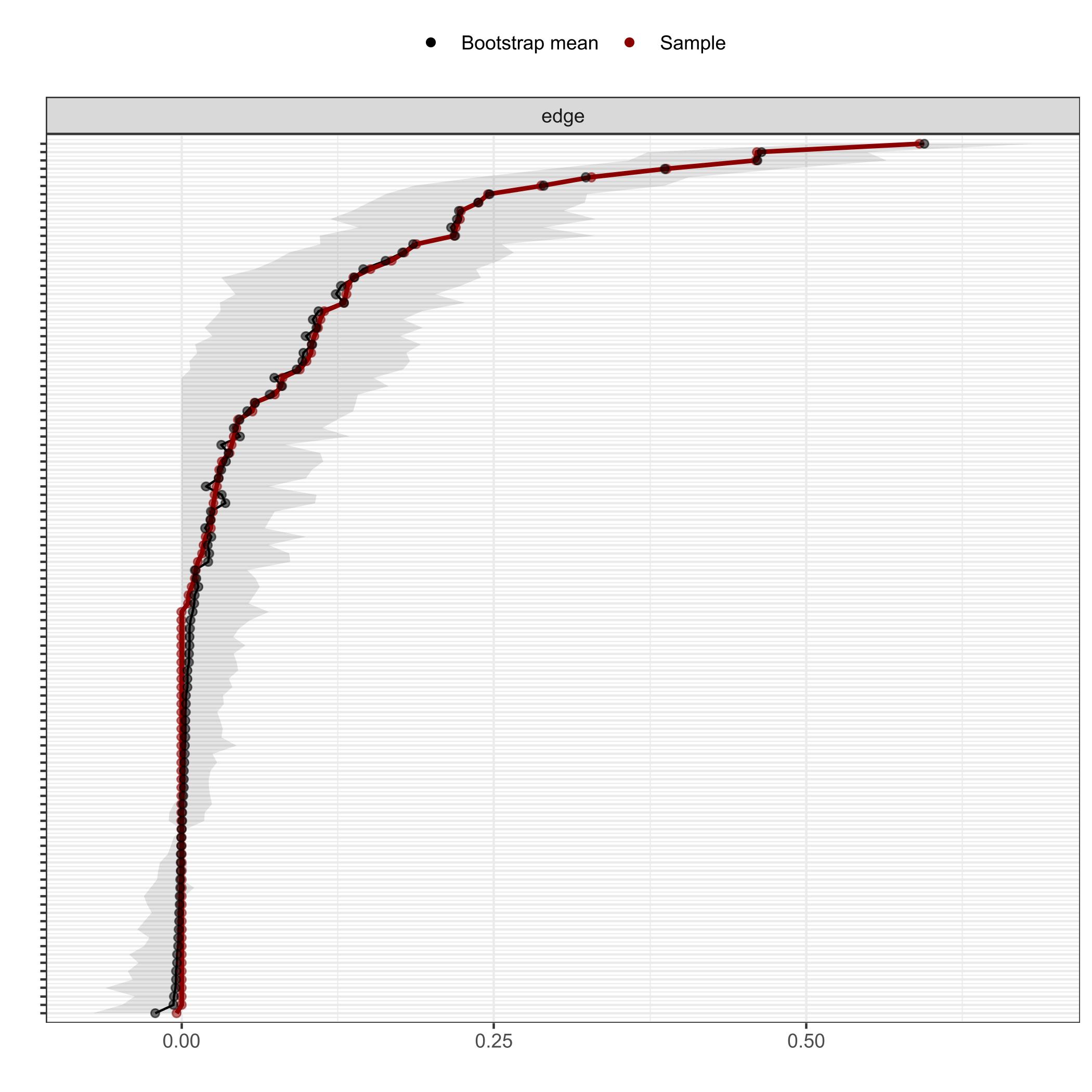
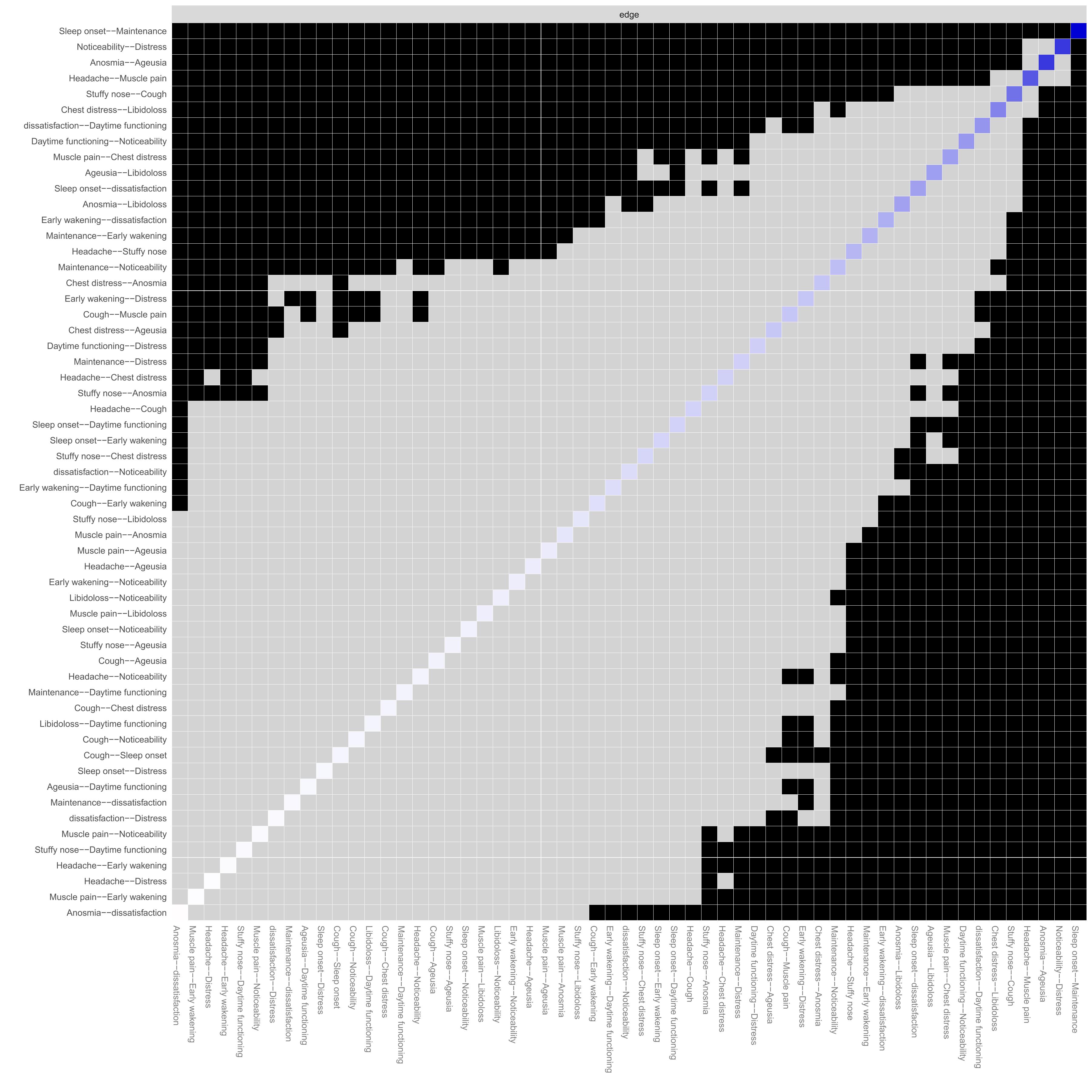
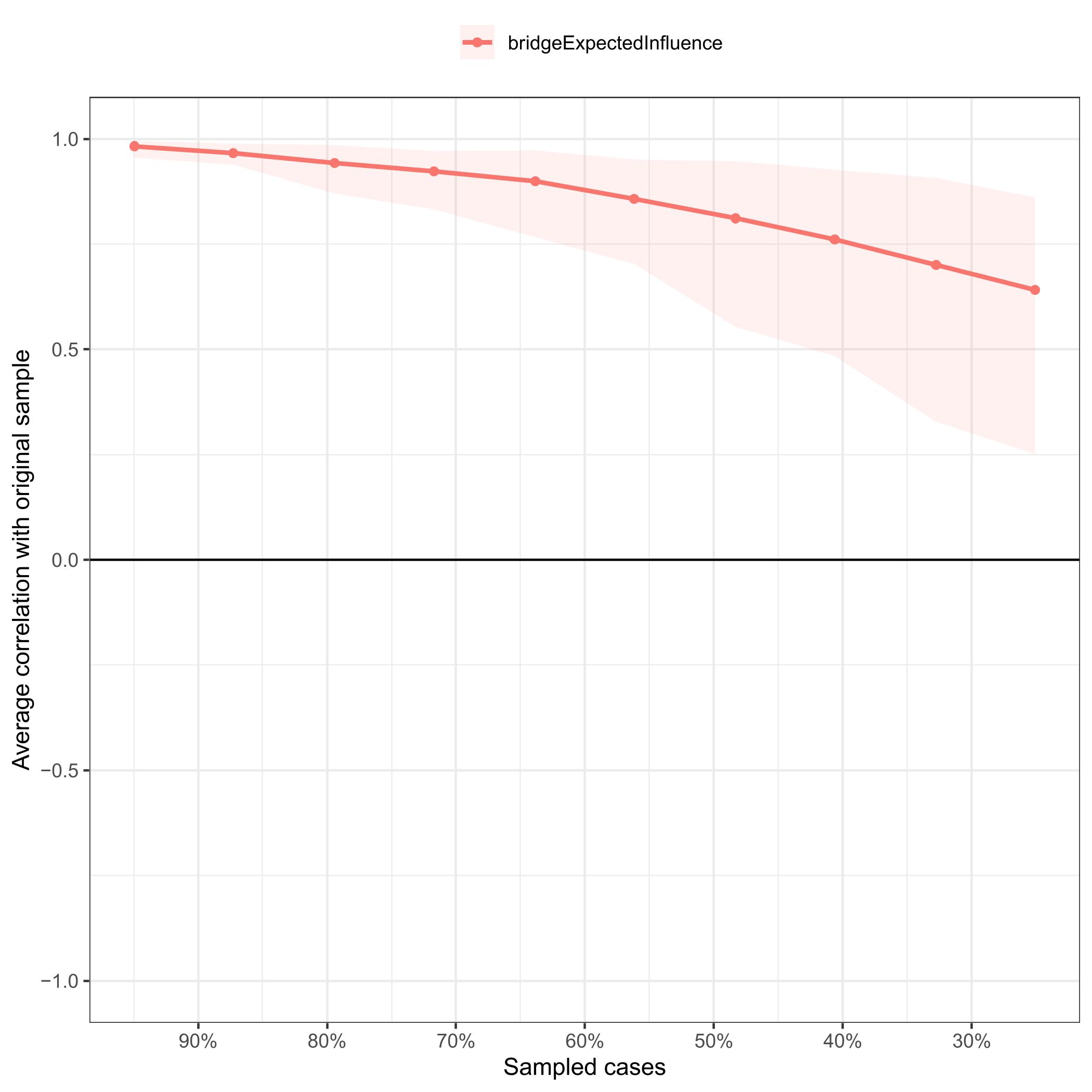
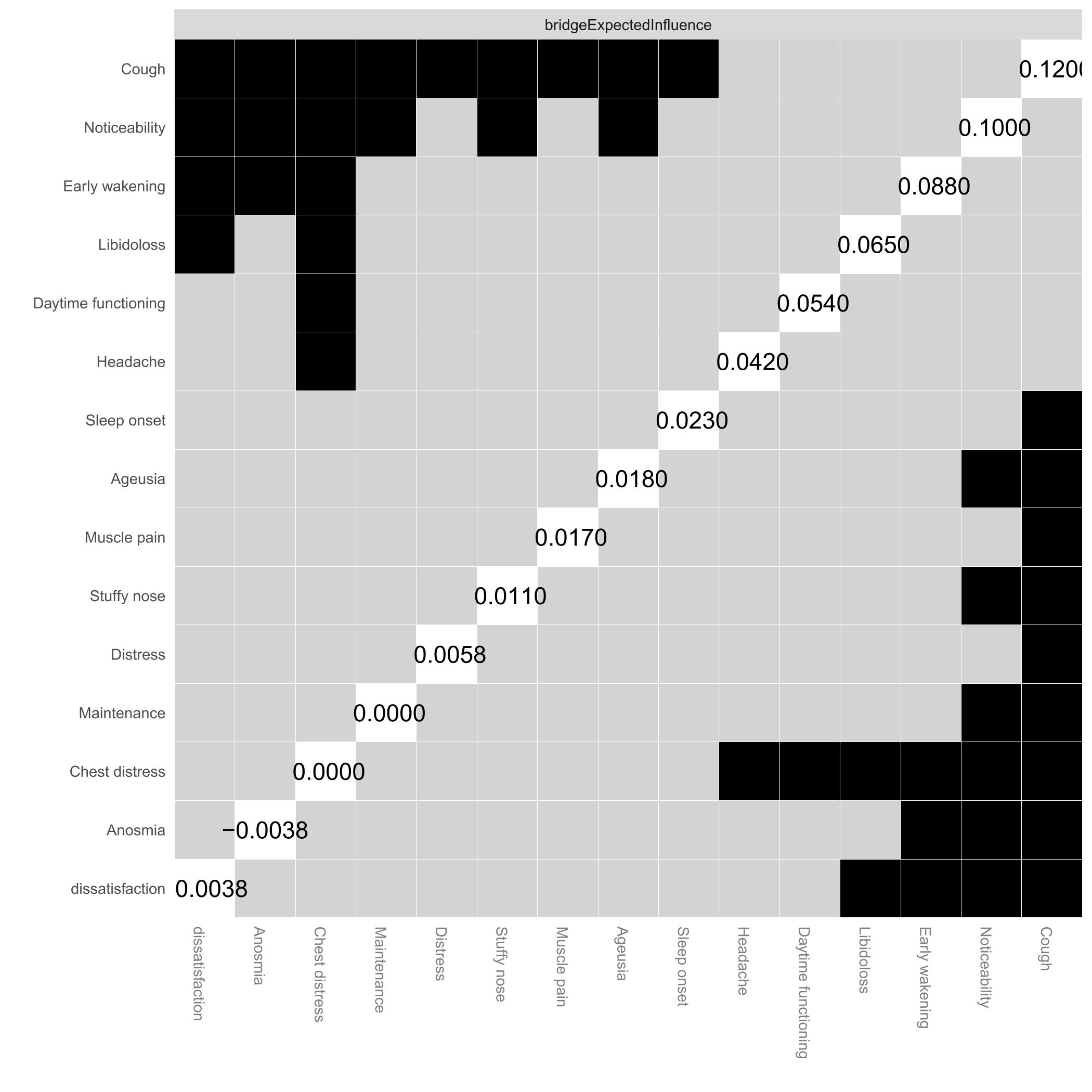
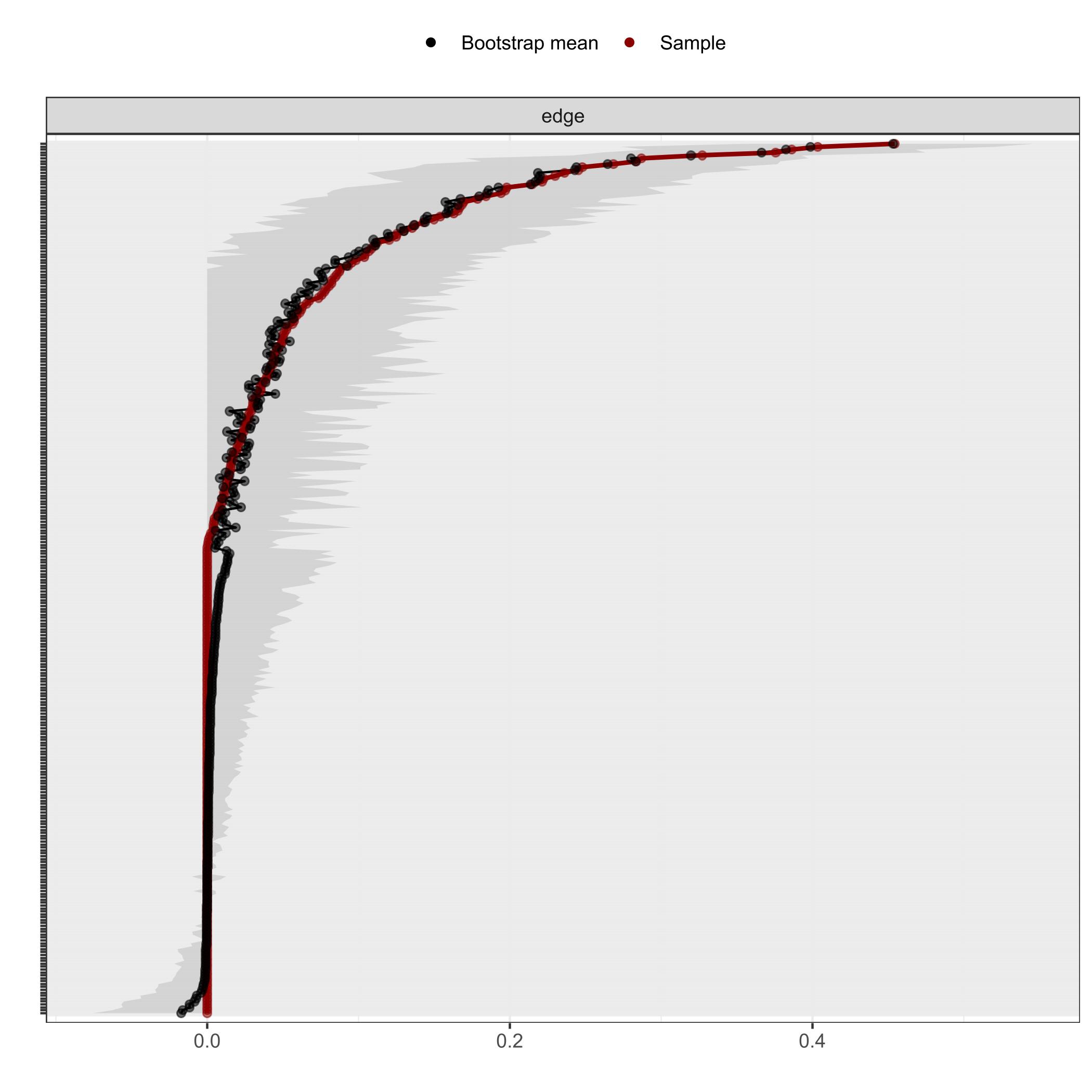
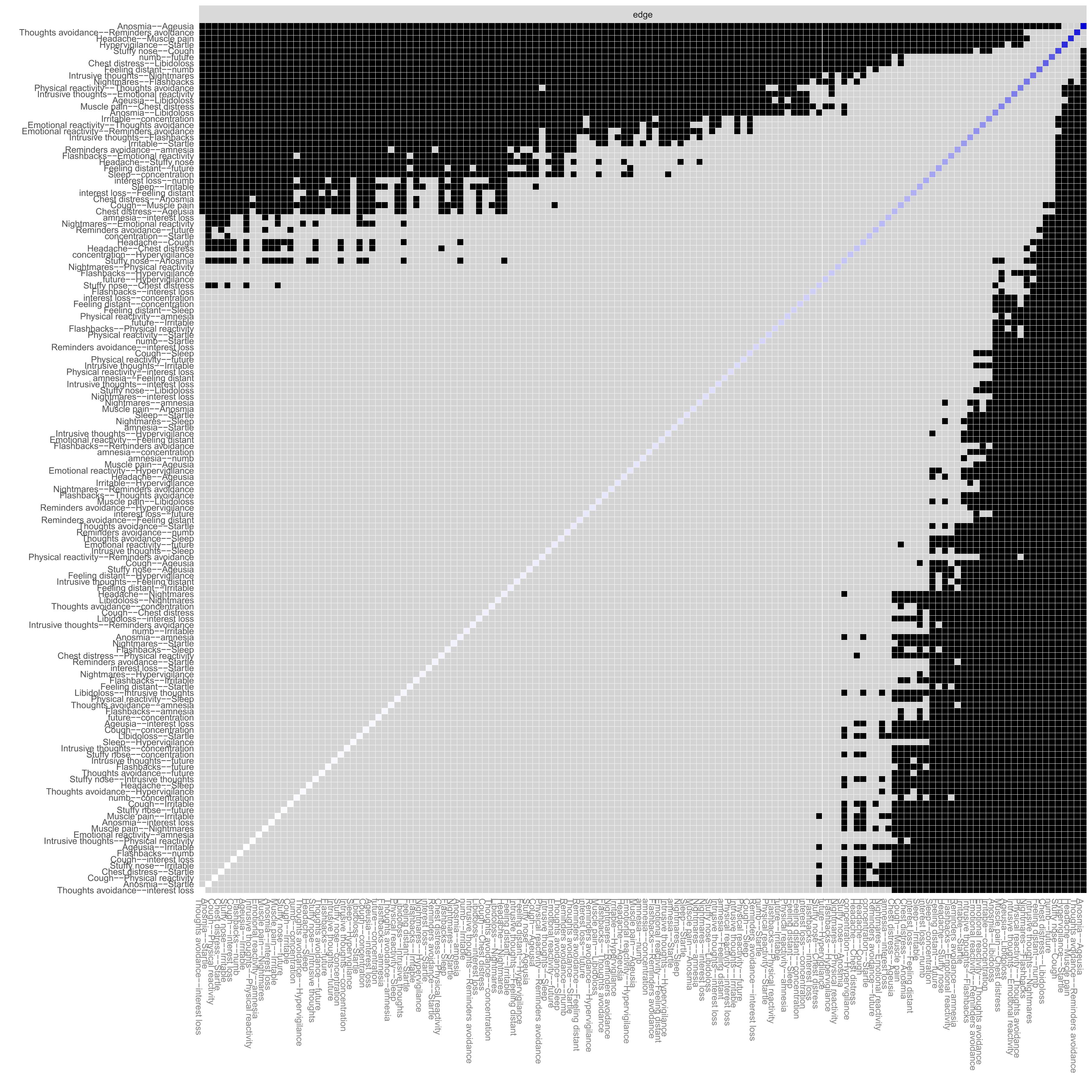
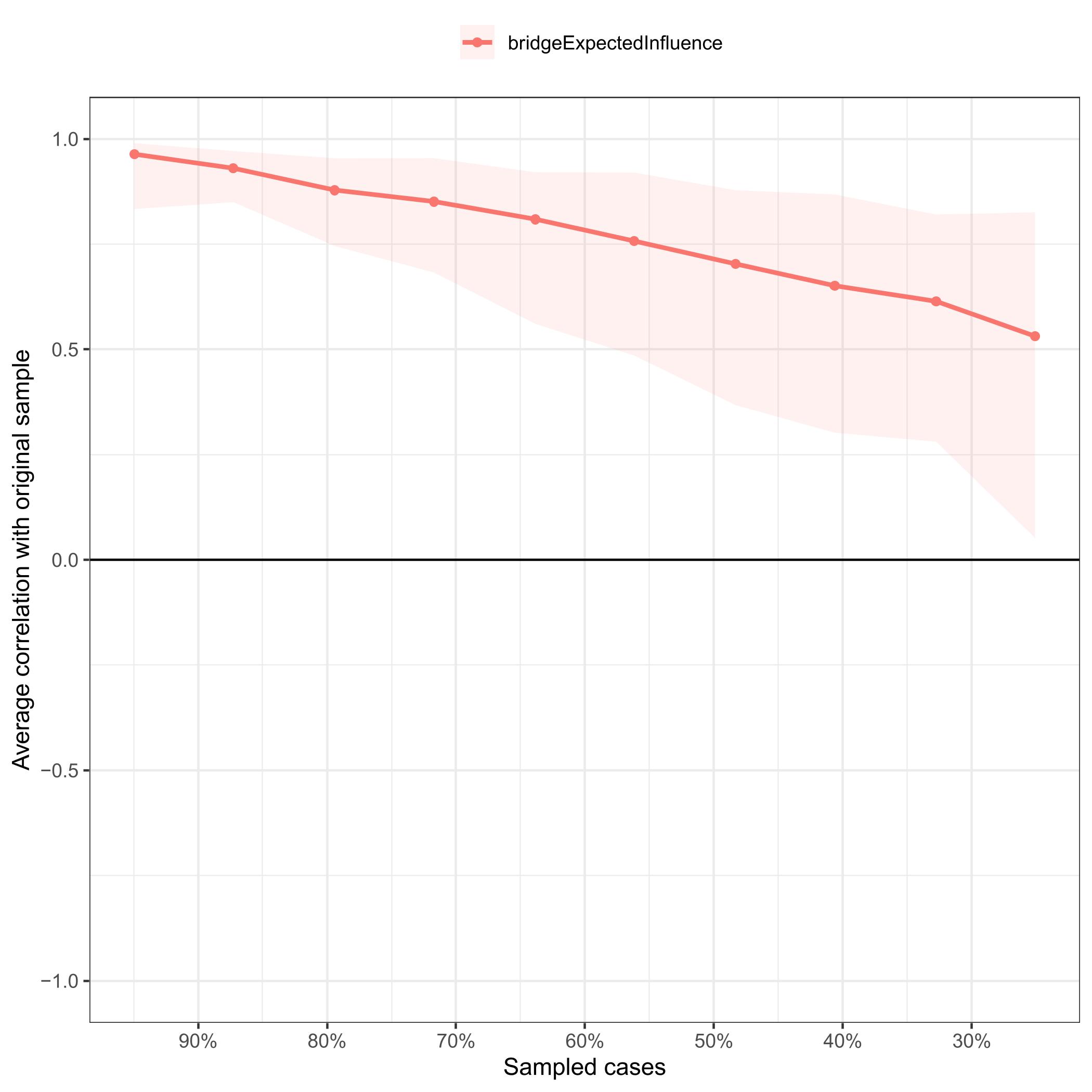
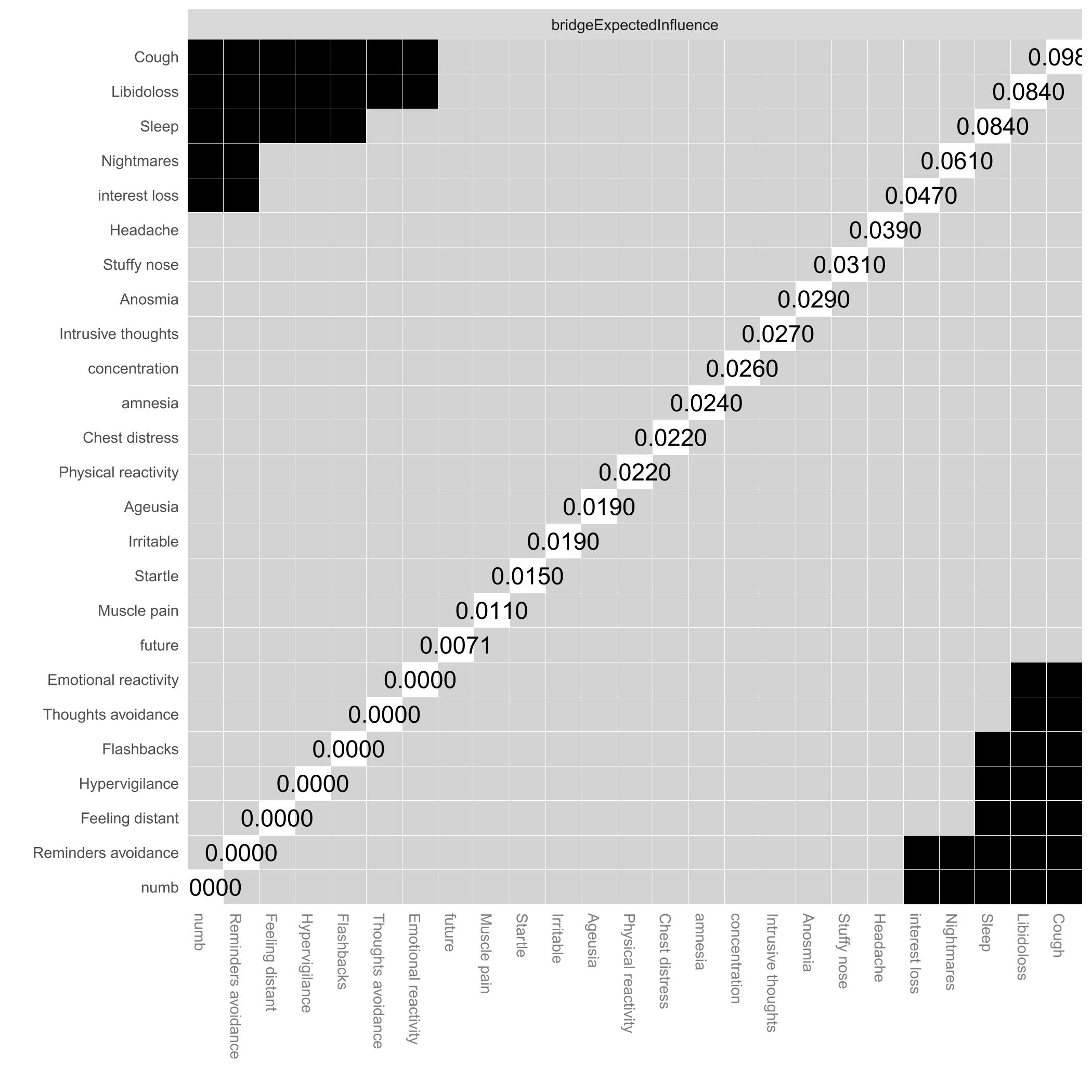
This study enrolled 534 Chinese COVID-19 inpatients revealed that COVID-19 inpatients were frequently accompanied by psychiatric manifestations such as depression, insomnia, and PTSD, with incidence rates of 100%, 77.63%, and 5.99%, respectively—significantly surpassing those in the general population [33] -[34]. A network model illustrating the intrinsic connections between somatic symptoms and depression, insomnia, and PTSD. In the depression-somatic symptom network revealed seven robust edges, including “Anosmia”-“Ageusia”, “Headache”-“Muscle pain”, “Stuffy nose”-“Cough”, “Cough”-“Anhedonia”, “Cough” - “Sleep”, “Cough”-“Fatigue”, and “Muscle pain”-“Fatigue”. The insomnia-somatic symptom network highlighted five robust edges, including “Sleep onset”-“Maintenance”, “Noticeability”-“Distress”, “Ageusia”-“Anosmia”, “Headache”-“Muscle pain”, and “Stuffy nose”-“Cough”. The PTSD-somatic symptom network featured five prominent edges, including “Ageusia”-“Anosmia”, “Headache”-“Muscle pain”, “Reminders avoidance”-“Thoughts avoidance”, “Hypervigilance”-“Startle”, and “Stuffy nose”-“Cough”. Simultaneously, “Cough”、“Anhedonia”、 “Noticeability”、“Libido loss” and “Sleep” play a crucial role as bridge factors linking somatic symptoms with psychiatric symptoms. Meanwhile, “Cough”、“Anhedonia”、 “Noticeability”、“Libido loss” and “Sleep” play a crucial role as bridge factors linking somatic symptoms with psychiatric symptoms.
Prior investigations have indicated the prevalence of depressive symptoms and major depressive disorder in patients with "Cough" [35]-[36]. In line with these findings, this study identifies "Cough" as a crucial bridge factor between somatic symptoms and depressive symptoms in hospitalized COVID-19 patients. This connection plays a role in regulating key nodes associated with depressive symptoms, including "Anhedonia," "Sleep," "Appetite," "Concentration," and "Fatigue," aligning with previous literature reports [37]. Examining the neurobiological mechanism underlying the mutual regulation of cough symptoms and depressive symptoms in COVID-19, cough induces an increase in gray matter nerve electrical activity around the aqueduct in the midbrain [38]-[39]. This activity is involved in regulating stress, pain, and depression, among other emotions [37]. Conversely, elevated blood cortisol concentrations and abnormalities in the hypothalamic-pituitary-adrenal cortical axis (HPA axis) following SARS-CoV-2 infection are identified as crucial contributors to depression [40]-[41]. Past studies have established that the severity of cough serves as an independent risk factor for depressive symptoms, show casing a bidirectional moderating relationship between cough and psychiatric symptoms such as depression and insomnia[42]-[43]. Besides, this study founds "Cough" as a crucial bridge factor between somatic symptoms and insomnia and PTSD symptoms in hospitalized COVID-19 patients. This relationship may be associated with pathophysiological processes such as abnormal gene expression in the prefrontal cortex and limbic system of the brain, increased synapse formation, and dendritic growth in the amygdala, along with dendrite contraction in the hippocampus. Additionally, inflammatory responses and autonomic nerve damage, resulting from physical diseases, psychological stress, and emotional trauma, could contribute to this intricate relationship [44]. The finding that "Anhedonia" serves as an additional connecting bridge factor between somatic symptoms and depressive symptoms in hospitalized COVID-19 patients is consistent with previous research. "Anhedonia" is an essential symptom in the diagnosis of depression, and previous research has demonstrated a strong relationship between headache, pleasure deficit, and depression[45].
"Noticeability" as another bridging symptom between insomnia and somatic symptoms, consistent with previous studies that insomnia is associated with headache[46], the present study further found "Noticeability" to be associated with headache, cough, muscle pain, and loss of libido.
"Libido loss" emerges as a pivotal bridging factor connecting somatic symptoms and PTSD symptoms, exhibiting associations with PTSD-related nodes such as "Intrusive thoughts," "Nightmares," "Interest loss," and "Startle." This finding aligns with existing literature suggesting that PTSD is linked to a heightened incidence of libido loss[47]. Earlier research has indicated that libido loss in individuals with PTSD may be linked to diminished plasma levels of dehydroepiandrosterone and cortisol, coupled with a weakened response to the dexamethasone inhibition test[48]-[49]. Consequently, the correlation between libido loss and PTSD could represent specific clinical manifestations of adaptive changes in response to stress [50]. Moreover, PTSD has been associated with the upregulation of pro-inflammatory factors like IL-1β, IL-6, and TNF-α, leading to immune dysfunction[51]. However, the potential relationship between this process and libido loss, as well as increased acute cardiovascular risk, warrants further investigation. In addition, the present study found "Sleep " to be another bridging symptom between PTSD and somatic symptoms, which is consistent with previous research that sleep in PTSD is associated with headache and loss of libido.
Limitations and strengths
While this study offers novel insights for disease assessment interventions, certain limitations must be acknowledged. Firstly, the cross-sectional nature of this study impedes the determination of a regulatory causal relationship between somatic symptoms and neuropsychiatric symptoms. Secondly, reliance on internationally accepted classical questionnaire scales introduces inherent subjectivity in patient responses.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}