A total of 254 children and adolescents with PHT were considered for inclusion, however only 174 could be finally included prospectively (Fig. 1). The median age (IQR) of the whole cohort was [10.0 years, IQR 2.4–14) with majority being males (n = 119, 68.4%). The median SSM and LSM by TE and SMM/LSM ratio were 29.5 (IQR 22-56.2) kPa and 26.5(IQR 11.7–42.0) kPa and 1.15 (IQR 0.8–2.23), respectively, in the whole cohort. The prevalence of CSV was 57.4%(n = 100) in the whole cohort, of which 18.9% (n = 33) were bleeders.
Children and adolescents with NCPF (n = 27)
Of the 27 children and adolescents with NCPF, most patients were male (76.2%). Specific histologic finds of the NCPF cohort included maintained lobular architecture (n = 27, 100%), atretic portal tracts (n = 27, 100%), abnormal approximation of portal-portal and portal-central vein (n = 23, 85.1%), partial and complete absence of central vein profiles (n = 15, 55.5%), sinusoidal dilatation (n = 13, 48.1%), nodular regenerative hyperplasia (n = 9, 33.3%), phlebosclerosis (n = 3,11.1%) (Table 1).
Table 1
Specific histologic findings associated with the diagnosis of NCPF (n = 27)
| Histologic findings | n (%) |
| Maintained lobular architecture | 27(100%) |
| Atretic portal tracts | 27(100%) |
| Abnormal approximation of portal-portal and portal-central vein | 23(85.1%) |
| Partial and complete absence of central vein profiles | 15(55.5%) |
| Sinusoidal dilatation | 13(48.1%) |
| Nodular regenerative hyperplasia | 9(33.3%) |
| Phlebosclerosis | 3(11.1%) |
Children and adolescents with cirrhosis
Of the 147 patients’ of CLD included (Fig. 1), again most of the patients were male 97(65.9%). Wilson disease was the most common (n = 41, 27.8%) etiology amongst all, followed by Biliary atresia (n = 36, 24.5%) and Auto immune liver disease (n = 32, 21.7%).
The baseline clinical and laboratory profiles of the children and adolescents with CLD and NCPF group are compared in Table 2. The median age of NCPF group (13.5 years, IQR 9.0–15.0) was significantly higher (p = 0.001) than the CLD group (9.0 years, IQR 1.7–14). Bleeders were significantly more (p < 0.001) in the NCPF group (n = 13, 48.1%) compared to CLD group (n = 20, 13.6%). Nutrition in terms of weight for height (WFH) z score (p = 0.022) and height for age (HFA) z score (p = 0.029) was significantly maintained in NCPF group relative to CLD group. Spleen size on ultrasound was significantly higher (p < 001) in the NCPF group (15.9 cms, IQR 12.8–17.6) compared to the CLD group (12.3 cms, IQR 9.6–15.2). Similarly, splenic z scores was also significantly higher (p < 001) in the NCPF group (7.38, IQR 4.55–8.58) compared to the CLD group (4.14, IQR 2.96–6.9). Amongst the laboratory investigations, patients with NCPF had lower levels of total leukocyte count (p < 0.001), platelet count (p = 0.001), while patients with CLD had higher median levels of bilirubin (p = 0.005), and prothrombin time (p = 0.021) compared to the CLD group at index presentation. CLD group had a significantly higher Pediatric End Stage Liver Disease (PELD) Score (p < 0.03) and Child Turcotte Pugh (CTP) score (p = 0.001) compared to the NCPF group (Table 2).
Table 2
Baseline clinical and laboratory parameters of the children with portal hypertension included in the study.
| Parameter | Total n = 174 Median(IQR) | CLD n = 147 Median(IQR) | NCPH n = 27 Median(IQR) | Odd’s ratio or Mean difference (95% CI) | p value |
| Age(yrs) | 10.0(2.4–14) | 9.0(1.7–14) | 13.5(9.0–15.0) | 3.02 (1.04–5.2) | 0.001 |
| Male n(%) | 119(68.4) | 97(65.9) | 22(81.5) | 0.018 (0.014–0.19) | 0.122 |
| WFH (Z-score) | -0.99(-2.4- 0.15) | -0.70(-2.1- 0.19) | -1.9(-2.8- -0.46) | 0.61 (0.23–1.23) | 0.022 |
| HFA (Z-score) | -0.94(-2.0- 0.30) | -0.75(-1.99- 0.50) | -1.3(-2.8- -0.86) | 1.12 (1.55–3.78) | 0.029 |
| Bleeder n(%) | 33(18.9) | 20(13.6) | 13(48.1) | 0.24 (0.09–0.49) | < 0.001 |
| Age index bleed (years) | 11.0(3.4–13.8) | 6.5(1.5–14.2) | 11.7(8.0-13.8) | 2.43 (1.94–6.9) | 0.149 |
| Spleen size USG (cm) | 12.5(10.2–15.9) | 12.3(9.6–15.2) | 15.9(12.8–17.6) | 3.2 (1.48–4.64) | < 0.001 |
| Splenic Z-score (SZS) | 4.47(2.4–7.1) | 4.14(2.96–6.9) | 7.38(4.55–8.58) | 2.26 (0.95–3.23) | < 0.001 |
| Laboratory Parameters |
| Bilirubin (mg/dL) | 1.8(1.07-5.0) | 2.1(1.1–6.8) | 1.3(1.0-2.4) | 4.38(1.3–7.4) | 0.005 |
| Albumin (g/dL) | 3.2(2.4–3.7) | 2.9(2.4–3.7) | 3.7(2.9–3.8) | 0.79(-0.64- 0.05) | 0.097 |
| INR | 1.34(1.1–1.8) | 1.37(1.1–1.8) | 1.30(1.1–1.4) | 0.28(0.11–0.45) | 0.021 |
| Hb (g/dL) | 10.4(9.1–11.8) | 10.6(9.1–11.8) | 9.6(8.9–11.4) | 0.72(-0.108- 1.55) | 0.088 |
| TLC (X10^3)/ cu.mm | 6.5(4.2–9.04) | 7.0(4.5–9.5) | 4.09(2.2–4.5) | 3.1(1.77–6.50) | < 0.001 |
| Platelet (X10^3)/ cu.mm | 109.5(65-169.2) | 114(80–148) | 102(52–148) | 41.2(28.0.-94.3) | 0.001 |
| PELD | 4.0(-3.7- 16.0) | 5.0(-3.0- 17.0) | 1.46(-5.0- 6.0) | 5.9(0.53–11.4) | 0.03 |
| CTP | 7.0(6.0–10.0) | 8.0(6.0–10.0) | 6.0(5.0–7.0) | 1.6(0.65–2.6) | 0.001 |
The endoscopic findings, transient elastography measurements liver (LSM), spleen (SSM), SSM/LSM index and portal hypertensive indices of the children and adolescents with CLD and NCPF group are compared in Table 3. Comparatively, SSM was significantly higher (p < 0.001) amongst the children with NCPH (32.0 kPa, IQR 26.0–75.0) than CLD (28.0 kPa, IQR 21.0–42.0). The LSM was significantly (p < 0.001) lower amongst the children with NCPH (8.0 kPa, IQR 5.0-10.2) than CLD (29.1 kPa, IQR 18.0–50.0). The prevalence of CSV was significantly (p = 0.01) more amongst the children with NCPH (n = 20,74.1%) than CLD (n = 80, 54.4%).
Table 3
Endoscopic features, transient elastography measurements (liver and spleen) and portal hypertensive indices of children with cirrhotic and non-cirrhotic portal hypertension.
| Parameter | Total n = 174 | CLD n = 147 | NCPH n = 27 | Odd’s ratio or Mean difference (95% CI) | p value |
| Endoscopic features |
| Esophageal varices n(%) | 141(81.03%) | 118(80.3%) | 23(85.2%) | 1.078 (0.480–2.315) | 0.572 |
| Grade 3 varices n(%) | 33(18.9%) | 24(16.3%) | 9(33.3%) | 1.842 (1.003–3.619) | 0.042 |
| Red colour signs | 50(28.7%) | 37(25.2%) | 13(48.1%) | 2.018 (1.081–3.788) | 0.022 |
| PHG | 115(66.1%) | 91(61.9%) | 24(88.9%) | 3.736 (1.185–11.880) | 0.007 |
| Gastric varices | 17(9.7%) | 9(6.1%) | 8(29.6%) | 2.881 (1.366–5.622) | 0.004 |
| CSV | 100(57.4%) | 80(54.4%) | 20(74.1%) | 0.192(0.008–0.41) | 0.01 |
| Transient elastography measurements (Liver and Spleen) |
| SSM (kPa) | 29.5(22-56.2) | 28.0(21.0–42.0) | 32.0(26.0–75.0) | -11.3(-19.7- -2.82) | 0.009 |
| LSM (kPa) | 26.5(11.7–42.0) | 29.1(18.0–50.0) | 8.0(5.0-10.2) | 27.86(19.17–36.55) | < 0.001 |
| SSM / LSM Index | 1.15(0.8–2.23) | 1.05(0.79–1.55) | 8.3(6.7–11.6) | -8.24(-9.10- -7.39) | < 0.001 |
| Portal hypertensive indices |
| EASS | 17.9(14.9-21.97) | 17.46(14.7-21.57) | 22.2(18.07–24.08) | -3.46(-5.2- − 1.63) | < 0.001 |
| KVaPS | 54.53(34.5–79.1) | 55.51(33.32–79.1) | 50.8(34.9–79.3) | -1.91(-13.7- 9.91) | 0.750 |
| VPS | 33.4(16.5–58.1) | 35.8(18.6–62.4) | 17.3(13.2–42.7) | 20.1(4.4-35.78) | 0.012 |
| CPR | 88.4(69.9-110.5) | 88.6(69.3-110.5) | 84.8(76.1-104.7) | 1.34(-9.88–12.58) | 0.81 |
| APRI | 2.2(1.1–4.6) | 2.5(1.13–5.34) | 2.09(0.87–3.31) | 13.06(-35.17- 61.3) | 0.59 |
Diagnostic performance of TE parameters in differentiating NCPF from CLD
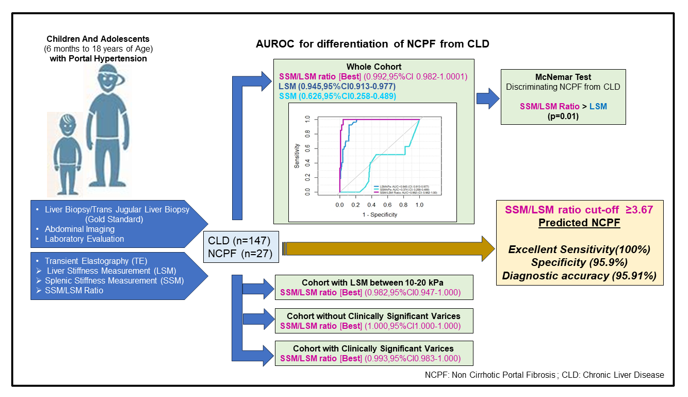
The AUROC of LSM, SSM and SSM/LSM ratio index for the diagnosis of NCPF were 0.945 (95% CI 0.913–0.977), 0.374 (95% CI 0.258–0.489) and 0.992 (95% CI 0.982-1.000) respectively in the whole cohort (Fig. 2a). Even on restricting the analysis to the patient cohort which is most controversial i.e. having LSM values from 10 to 20 kPa (n = 36; 8 in NCPF group), SSM/LSM remained an excellent predictor for the diagnosis of NCPF with an AUROC of 0.982 (95% CI 0.949-1.000) unlike LSM whose AUROC of decreased to 0.848 (95% CI 0.695-1.000) in this subgroup (Fig. 2b). AUROC of SSM was good and better than LSM in this subgroup at 0.853 (95% CI 0.697-1.000) (Fig. 2b). To match the severity of PHT between NCPF and CLD groups, diagnostic accuracy of SSM, LSM and SSM/LSM ratio were also assessed in patient cohort sub groups without CSV and with CSV separately. In the cohort without CSV i.e. less severe PHT, AUROC of SSM/LSM was excellent (1.000, 95% CI 1.000–1.000) and much better than LSM (0.913, 95% CI 0.843-992) and SSM (0.864, 95% CI 0.752–0.976) (Fig. 2c). In cohort with CSV i.e. more severe PHT, AUROC of SSM/LSM ratio (0.993, 95% CI 0.983-1.000) was excellent and outperformed LSM (0.977, 95% CI 0.953-1.000 (Fig. 2d). The AUROC of SSM (0.472, 95%CI 0.286-658) was poor in patients with CSV (Fig. 2d).
LSM with a best cut-off value of 11.4 kPa, predicted the diagnosis of NCPF with a sensitivity of 88.5%, specificity of 92.6%, positive predictive value of 98.5%, negative predictive value of 59.5%, positive likelihood ratio of 11.93 and diagnostic accuracy of only 81.1% (Table 4). While SSM with a best cut-off value of 28.0 kPa predicted the diagnosis of NCPF with a poor sensitivity of 54.5%, specificity of 51.8%, positive predictive value of 86.02%, negative predictive value of 17.30%, positive likelihood ratio of 1.13 and diagnostic accuracy of 6.27% (Table 4). However, SSM/LSM ratio with best cut-off value of 3.66 predicted the diagnosis of NCPF with an excellent sensitivity of 100%, specificity of 95.9%, positive predictive value of 81.8%, negative predictive value of 100%, positive likelihood ratio of 24.5 and diagnostic accuracy of 95.91% (Table 4). The best cut-off value of 3.66 of SSM/LSM ratio as obtained for the whole cohort was applied and evaluated for diagnostic accuracy in the subgroups of patients i.e. patient cohort having LSM values from 10 to 20 kPa, patient cohort sub groups without CSV and with CSV, separately (Table 4). Even in the patient cohort having LSM values from 10 to 20 kPa, which is considered as the most difficult to diagnose group, cut-off value of 3.66 of SSM/LSM ratio predicted the diagnosis of NCPF with a sensitivity of 100%, specificity of 66.7%, positive predictive value of 85.7%, negative predictive value of 100%, positive likelihood ratio of 3.0 and diagnostic accuracy of 88.88%. In the patient cohort sub group without CSV i.e. less severe PHT, it predicted the diagnosis of NCPF with a sensitivity of 100%, specificity of 70.0%, positive predictive value of 95.1%, negative predictive value of 100%, positive likelihood ratio of 3.3 and diagnostic accuracy of 95.58%. While in the patient cohort sub group with CSV i.e. more severe PHT, it predicted the diagnosis of NCPF with a sensitivity of 100%, specificity of 86.9%, positive predictive value of 95.9%, negative predictive value of 100%, positive likelihood ratio of 7.66 and diagnostic accuracy of 95.58% (Table 4).
Table 4
Diagnostic performance of TE measurements for discriminating NCPF from CLD (n = 174).
| Elastographic Measurement | AUROC (CI) | Cut off | p value | Se % | Sp % | PPV% | NPV% | +LR | -LR | Diagnostic Accuracy |
| LSM (n = 174) | 0.945 (0.913–0.977) | 11.4 kPa | < 0.001 | 88.5 | 92.6 | 98.5 | 59.5 | 11.93 | 0.12 | 81.1% |
| SSM (n = 174) | 0.374 (0.258–0.489) | 28.0 kPa | 0.015 | 54.5 | 51.8 | 86.02 | 17.30 | 1.13 | 0.87 | 6.27% |
| SSM/LSM (n = 174) | 0.992 (0.982- 1.000) | 3.67 | < 0.001 | 100 | 95.9 | 81.8 | 100 | 24.5 | 0 | 95.91% |
| SSM / LSM (LSM 10-20kPA) (n = 36) | 0.982 (0.949–1.016) | 3.67 | < 0.001 | 100 | 66.7 | 85.7 | 100 | 3.0 | 0 | 88.89% |
| SSM / LSM (CSV Absent) (n = 74) | 1.0(1.0–1.0) | 3.67 | < 0.001 | 100 | 70 | 95.1 | 100 | 3.33 | 0 | 95.58% |
| SSM / LSM (CSV Present) (n = 100) | 0.993 (0.983- 1.00) | 3.67 | < 0.001 | 100 | 86.9 | 95.9 | 100 | 7.66 | 0 | 96.77% |
On comparing the diagnostic accuracy of LSM (90.8%) with SSM/LSM ratio (95.97%) for differentiating NCPF from CLD using McNemar test, this difference was found to be statistically significant(p = 0.01) in favour of SSM/LSM ratio(Table 5).
Table 5
Comparison of Diagnostic performance of SSM/LSM Ratio and LSM for discriminating NCPF from CLD using McNemar test (n = 174)
| | LSM (Cut off 11.40) | | |
| Correct Diagnosis | Incorrect Diagnosis | Total | P value |
| SSM/LSM Ratio (Cut Off 3.66) | | | | |
| Correct Diagnosis | 128(73.6%) | 27(15.5%) | 155(89.1%) | 0.01 |
| Incorrect Diagnosis | 4(2.3%) | 15(8.6%) | 19(10.9%) | |
| Total | 132(75.8%) | 42(24.1%) | 174 | |
{kind=link}