Study Design and Participants
Data of this study were obtained from the Physical Examination System of Community Health Service Center. Free medical physical examination services are provided annually to community-dwelling people aged ≥ 60 years in Shanghai, China. We obtained the electronic medical records of health examinations from the Physical Examination System in 2018,2019,2020,2021. Given the focus of this study, we assembled a cohort, with participants who being not with AF in 2018 eligible for the baseline study and has no history of AF before. Follow-up was conducted in 2019, 2020, 2021 and new-onset AF during follow-up was recorded. New-onset AF adjudicated by a standard 12-lead electrocardiogram at a core laboratory reading center. Therefore, using the physical examination data from 2018 to 2021, we analyzed the relationship of satin prescription with new-onset in both stain users and nonusers. Then we explore the risk factors of new-onset AF in the elder people. All procedures were performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Shanghai Pudong Hospital, Fudan University. Written consent was obtained from each participant after they had been informed of the objectives, benefits, medical items, and confidentiality of personal information.
Participants were eligible for the study if they (1)were ≥ 60 years old, (2) had a Shanghai household registration or were resident in this community for more than three years,(3)without AF or AF history and (4)had complete baseline data in 2018 and 12-lead electrocardiogram at a core laboratory reading center in 2019,2020,2021.Exclusion criteria included (1) with AF in 2018 and a history of AF,(2) incomplete baseline data provided in 2018,(3)presence of severe mental illness, cognitive impairment or malignant tumors in 2018, and (4) incomplete 12-lead electrocardiogram at a core laboratory reading center provided in 2019,2020,2021(Fig. 1)
Data Collection and Outcome Measures
For each patient, comprehensive data were extracted from electronic medical records. Medical records included participant demographics (age and sex), body mass index (BMI), waist-to-hip ratio(WHR), systolic blood pressure (SBP) and diastolic blood pressure (DBP), history of smoking and drinking. We also collected information on participant clinical data ( including the prescription of angina-ten, sin-converting-enzyme inhibitor/angiotensin receptor blockers[ACEIs/ARBs]), calcium channel blockers[CCBs], beta-blocker, diuretics, and antidiabetic drugs, and medical history of hypertension and diabetes mellitus) and laboratory data (including glycated hemoglobin [HbA1c], fasting plasma glucose[FPG], total cholesterol [TC], triglyceride [TG], high-density lipoprotein [HDL], low-density lipoprotein [LDL], aspartate transaminase [AST], alanine transaminase [ALT],blood urea nitrogen[BUN],total bilirubin[TBIL],uric acid [UA] and serum creatinine [Scr] ), Neutrophil percentage(N%), Lymphocyte percentage(L%).
New-onset AF was defined as 12-lead electrocardiogram test manifested with AF in the follow up year and had no history of AF.
Statistical analysis
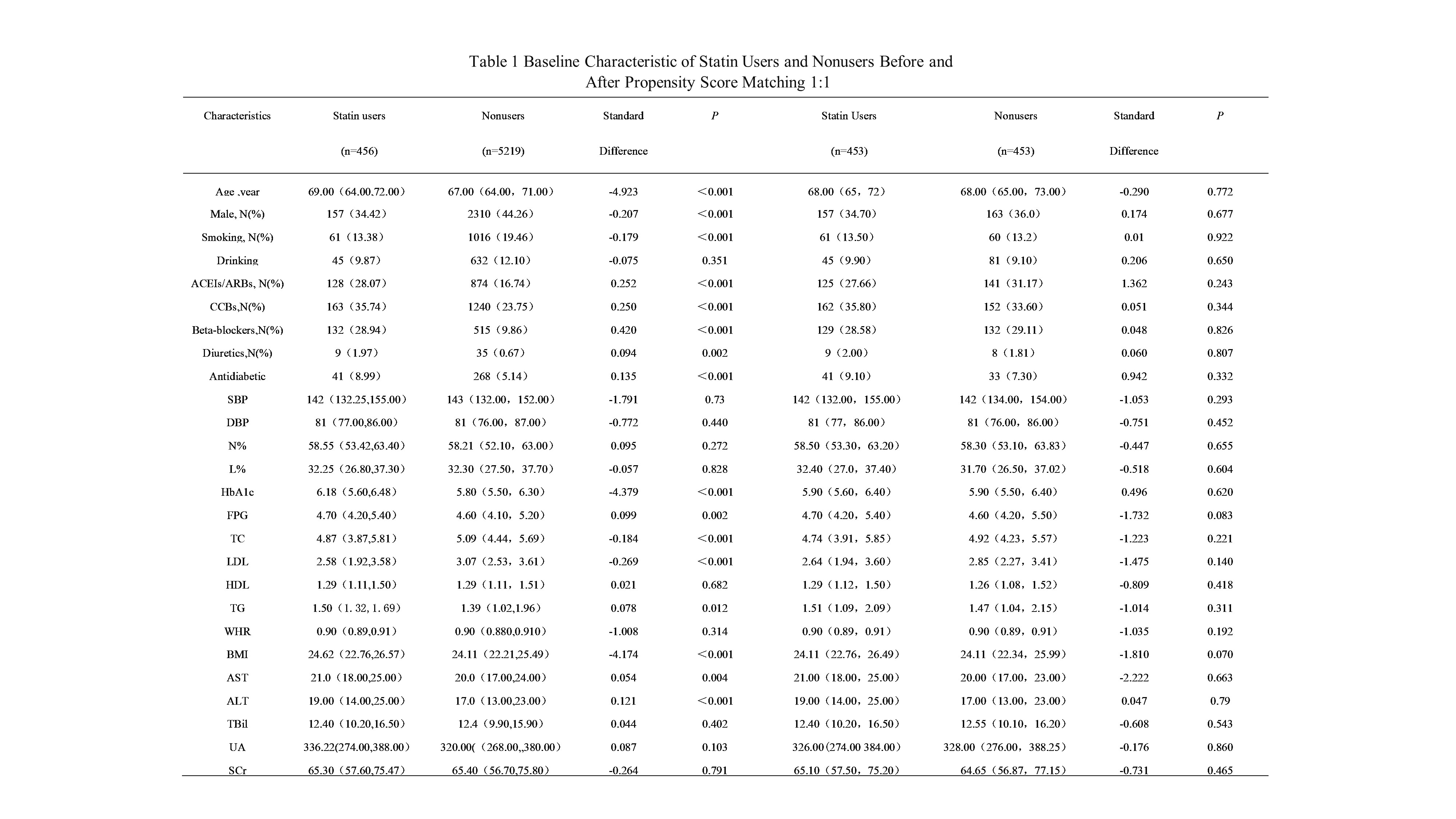
To reduce potential confounding and selection bias, we use the propensity score-matching method. propensity scores were calculated through a logistic regression model, with statin users versus nonusers as the dependent variable and covariates measured at baseline as independent variables(Table 1). Matched pairs were obtained using a greedy nearest-neighbor matching algorithm(1:1 ratio, without replacement ) and with a caliper width equal to 0.2 of the SD of the logit of the propensity score. A standardized difference of less than 0.1 was used to indicate a negligible difference in covariates between the groups.
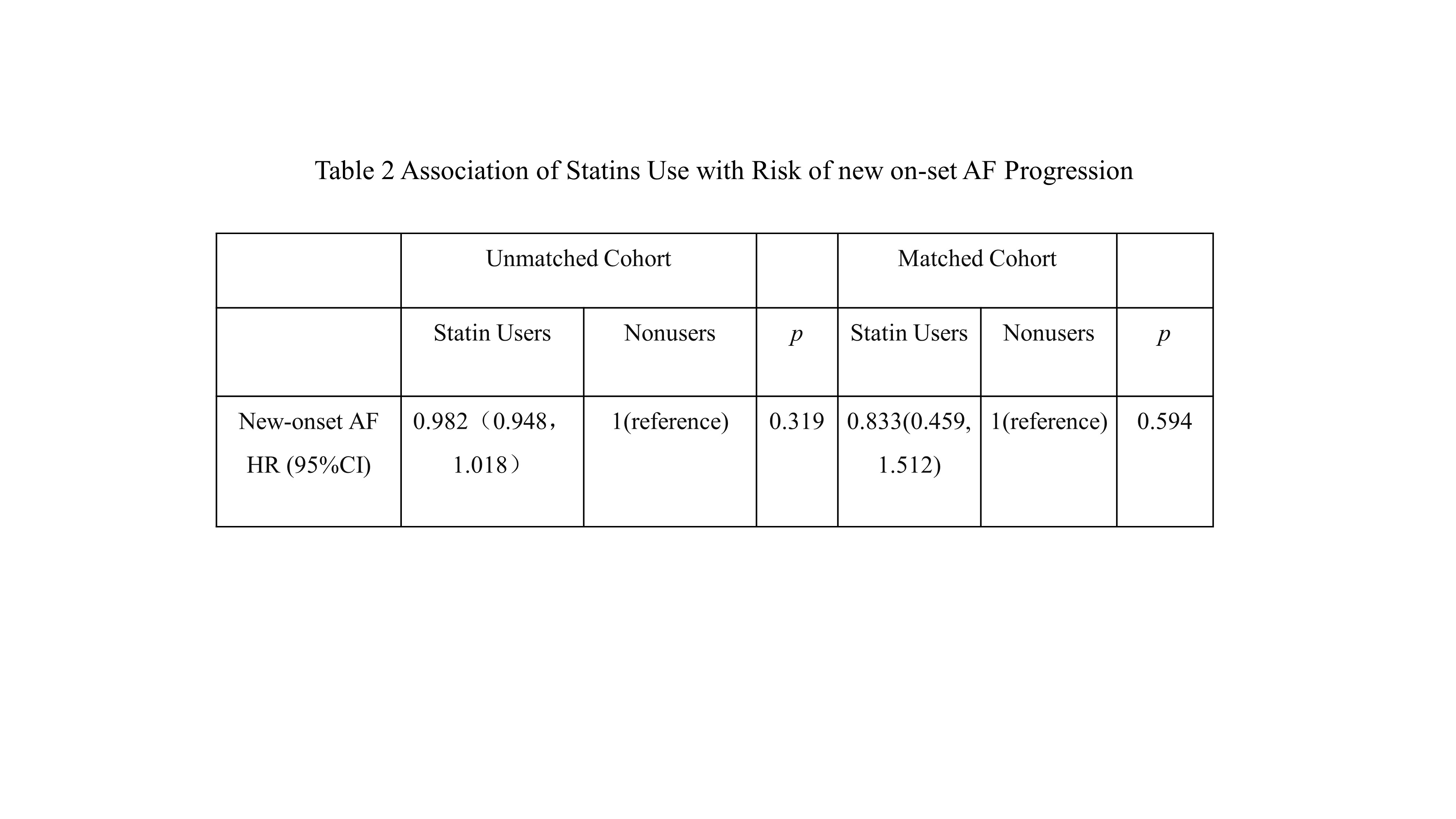
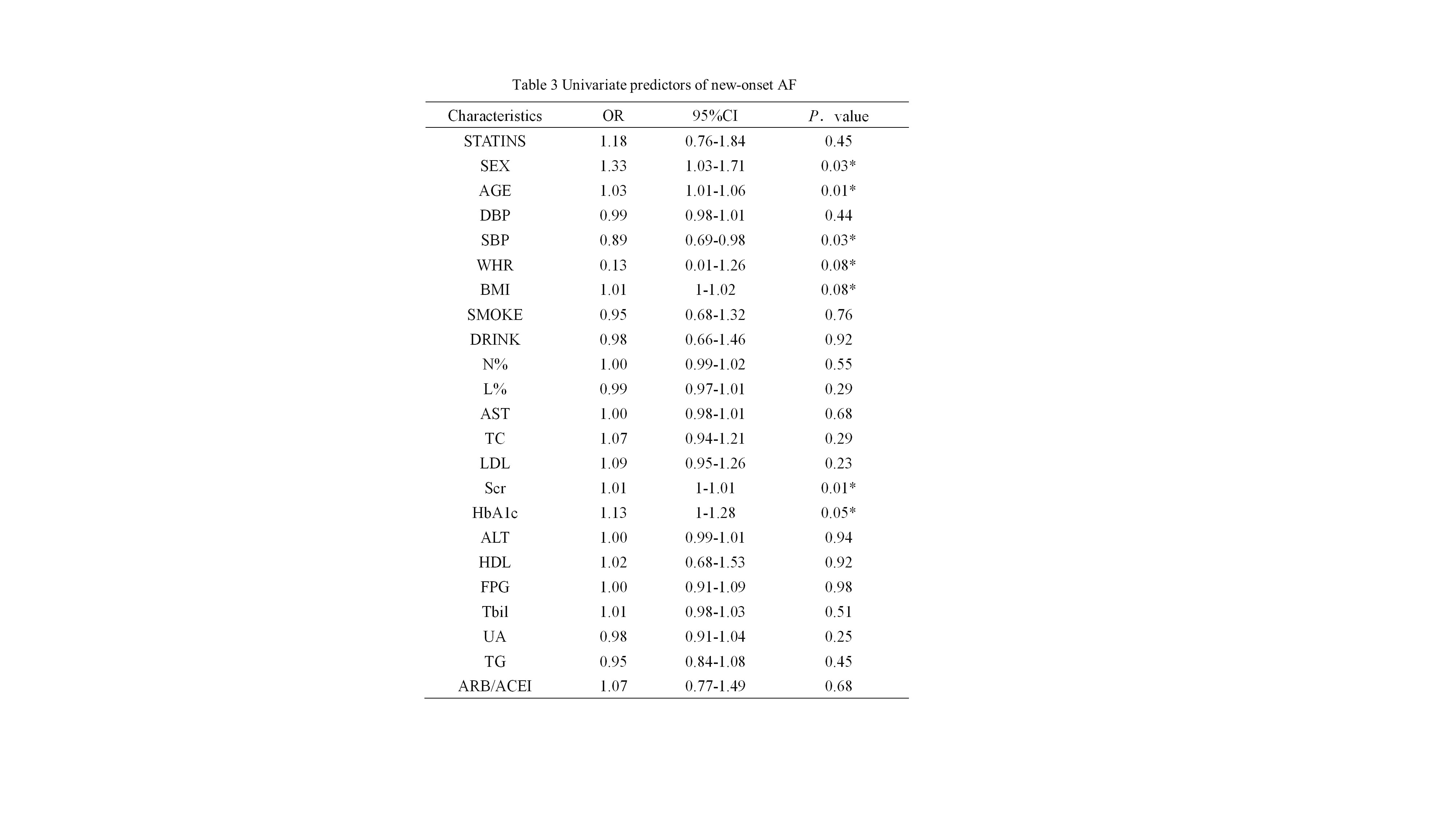
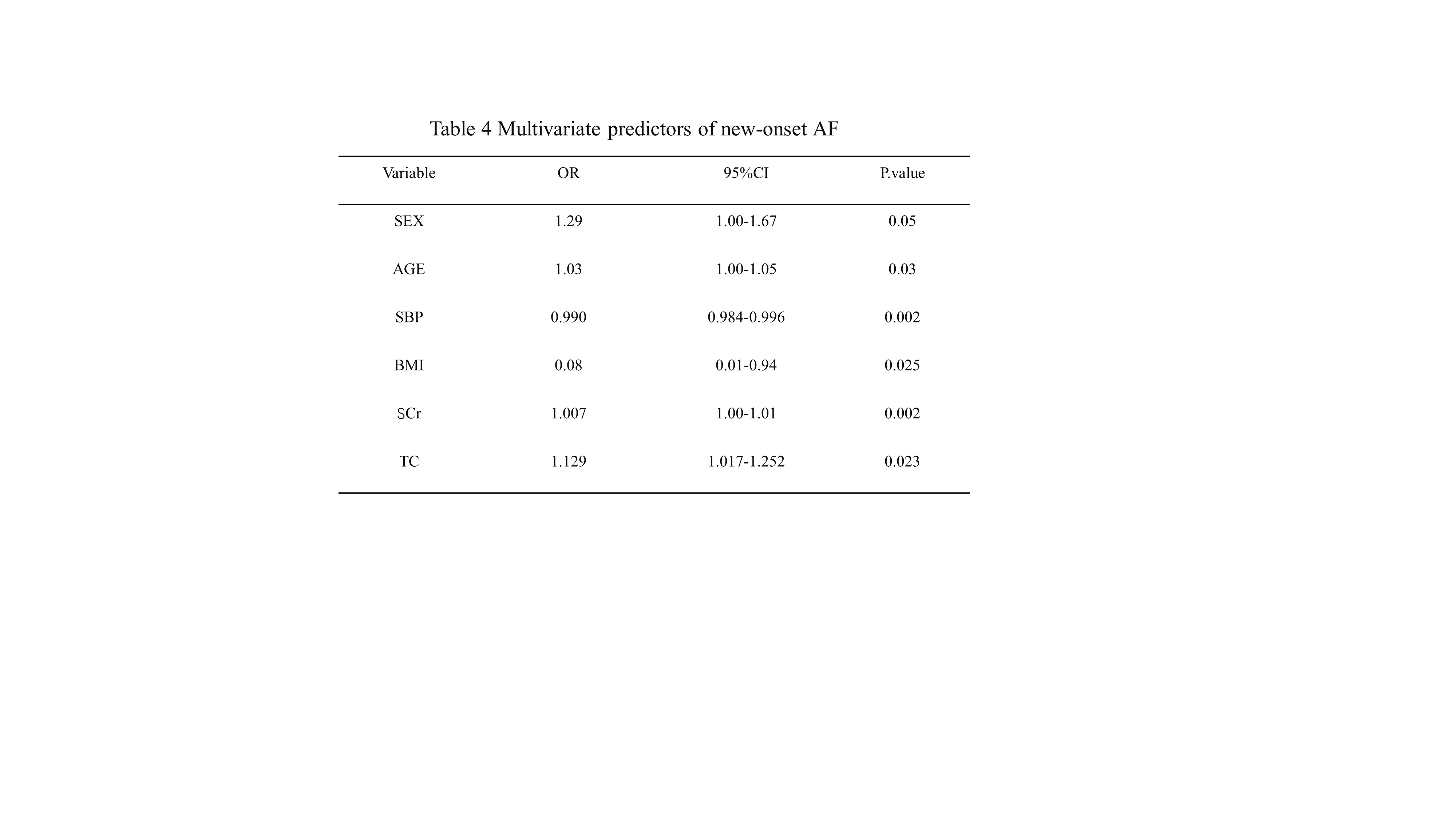
Poisson generalized linear models were conducted to explore the association between statin use and new-onset AF rates. Univariate binary logistic regression analysis(P<0.1 was considered as significant) and multivariate logistic regression analysis (P<0.05 was considered as significant)were performed to test the predictor of the new-onset of the community dwelling older people. Statistical analysis was performed by SPSS (NY, USA).
{kind=link}
{kind=link}
{kind=link}
{kind=link}