Our findings indicate that using a tourniquet and/or general anesthesia can effectively increase peripheral vein width. However, retroflexion of 30° or max° does not have any effect on vein width in supine patients. Previous studies have not thoroughly analyzed the impact of upper limb retroflexion with tourniquet application and its effect on vein width while in the supine position. Additionally, this is the first study to include patients in both awake and anesthetized states in its analysis.
Only one earlier work by Cappelletti et al showed an increase in the diameter and area of peripheral cephalic and basilic veins in healthy, awake subjects in the supine position with the arm dangling at a 90° angle compared with 0° [18]. This contrasts sharply with our findings, possibly due to varying study conditions.
First, our maximum position was less retroflexed (65-90°) compared with a dangling arm. Cappelletti et al. analyzed solely awake patients, in consideration of the potentially increased risk of plexus affection, especially in anesthetized patients, we avoided a dangling arm [15]. This should be considered in particular, as our awake evaluation of possible max retroflexion revealed, that 90° retroflexion cannot be achieved without paresthesia by most patients. Additionally, our work has shown a strong effect of the tourniquet. Therefore, it seems unlikely that gravity would have resulted in a significantly different effect for an arm bent backward 75° compared to an arm dangling 90°.
Second, the measurements were performed in a more proximal position compared to our CeV measurements, resulting in different baseline vein widths. An evaluation by Yamagami et al. showed a larger baseline diameter than our CeV results at different measurement sites [11]. Thus, different heights at the upper limb for measurement and lower consistency of the specific measurement point, compared to our setting, may further explain differences in baseline widths and results [8, 19].
Furthermore, heat affects vein width, as peripheral vein width may also be affected by different room temperatures. This is reflected by larger baseline results in studies with slightly higher OR temps of 22-24°C, compared to our setting [20, 21]. Besides room temperature, local warming or tapping are other, previously reported measures that can influence vein size [6, 8, 20, 22]. It is uncertain whether these measures would affect our results for retroflexion. However, we avoided them to ensure the comparability of the measures evaluated.
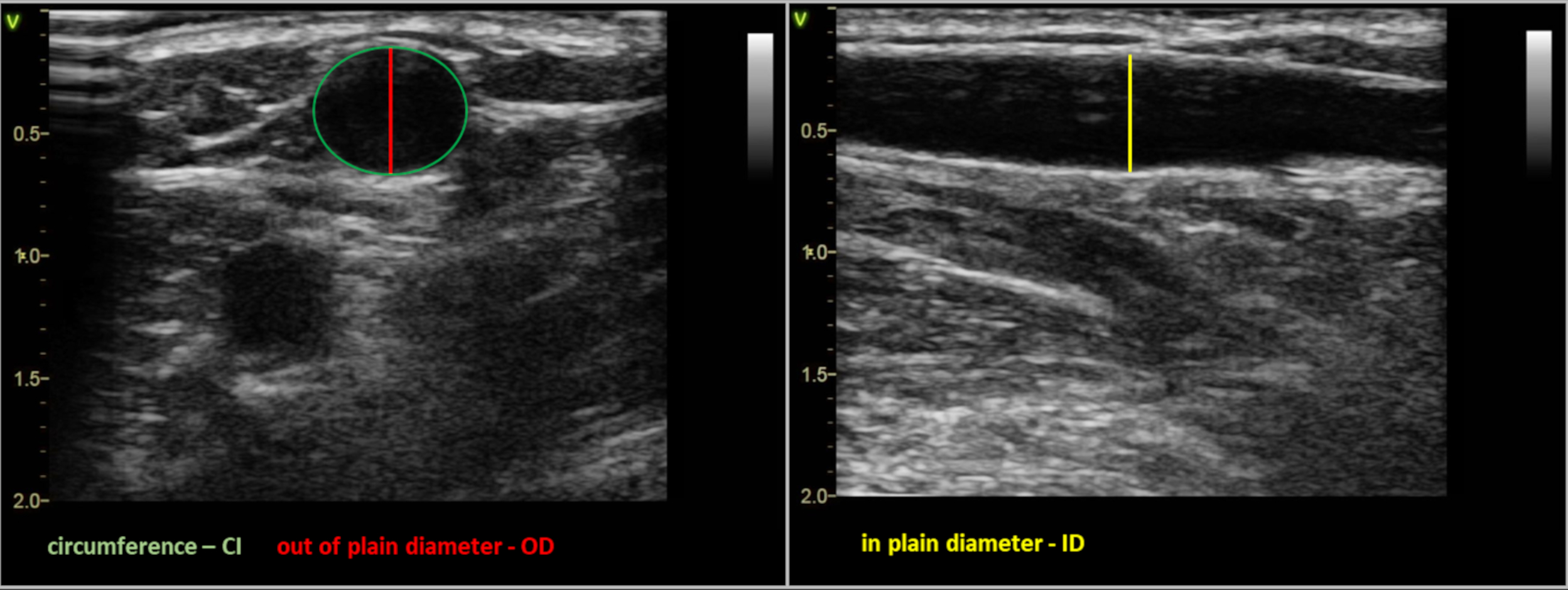
Our in-plane measurements agree with the out-of-plane measurements and can thus be considered as a validation of our measurement procedures (Supplemental Fig.2-3). This good correlation between the different measurement approaches indicates that differences in skin pressure with the probe, which could lead to possible vein deformation, were effectively avoided.
In contrast to many previous works that analyzed the effects on vein width only in healthy volunteers, our study is the first to examine patients before and after induction of anesthesia [8, 10-12, 18-20, 22]. GA, and especially propofol, is known to decrease peripheral vascular resistance after induction [23]. For this reason, in a clinical setting, often a small IV is first placed followed by a larger IV after anesthesia induction. Our findings confirm this effect of GA on peripheral vein widths. Additionally, gravidity-associated retroflexion revealed no further relevant enlargement, particularly in anesthetized patients, even when applying a tourniquet.
In contrast to healthy volunteers, all our patients were fasted before surgery, which may affect venous filling, especially since fasting has been discussed as a cause of difficult venipuncture [24, 25]. Previous research revealed controversial results regarding venous filling and reduced fluid intake during fasting. One study showed an increase in the cross-sectional diameter of the vena cava inferior after oral hydration in fasted patients [26]. Sharp et al demonstrated a reduction in forearm vein diameter after rehydration in fasting patients and discussed sympathetic nervous system activation as a possible cause [20]. Given these published controversial results, we administered fluids only at induction of general anesthesia and mostly in a "mild" form of less than 2 ml/kg body weight. Positive pressure ventilation can also act like a Valsalva maneuver and thus affect vein width [27]. In our study, the respiratory settings were within ranges considered normal, without particularly increased respiratory pressures, and were not altered during measurements for individual patients.
We chose to evaluate patients in the supine position because it is the usual position for IV access before general anesthesia as well as in pre- and intrahospital emergencies [5, 28]. It has also been demonstrated that the size of the veins appears to be larger in the supine position than in the seated position [11].
Furthermore, all measurements in our work were performed within a short period with comparable baseline conditions, which underlines the pronounced effect of tourniquet application.
Previous results showed the use of a blood pressure cuff had the greatest effect on increasing vein size and decreasing vein compressibility compared to other tourniquet techniques [29]. Sasaki et al. demonstrated an optimal effect of a blood pressure cuff on peripheral vein size enlargement when the cuff was inflated to a pressure of 60mmHg and applied for 30-60 seconds. After this time, there was no further increase in vein size [10]. According to these previous findings, our patients remained in each condition for 60 seconds before measurements were performed and the strong effect of tourniquet application was confirmed in our work.
Limitations of the study
It is known that vein width is influenced by gender [30], which was not explicitly analyzed in this work. Nevertheless, male and female participants were equally distributed in this work.
For reasons of patient comfort as well as to avoid impairment of vein width by multiple punctures, cannula insertion at the measured extremity was omitted in all cases. IV puncture success was not measured and can only be estimated by vein width [3, 4].
{kind=link}
{kind=link}
{kind=link}