The impact of health education interventions on breast cancer knowledge and awareness and cultural acceptable practices within underserved communities were explored in this study.
The overall knowledge score was very low in the baseline across all categories with few exceptions and only 16.5% manifested good knowledge. This study is in consonance with a similar studies conducted in Eastern China in which 18.6% of women aged 25–70 years had poor awareness of breast cancer (18). Similarly, this study’s findings concur partly with the southwest Ethiopian study in which more than 80% of the study participants did not know about breast cancer and BSE. Young adult women were less concerned about breast cancer and had insufficient knowledge of breast cancer and breast self-examination. (19). It is important to note that women in the above study were not expose to any health education intervention and the information given is only based on the baseline data.
The knowledge and awareness level has remarkably improved from 16.5% at the baseline to 61.3% after the health education intervention across all the participants. This increase in knowledge score was associated with the health education interventions conducted within 3 months after the baseline. Furthermore, women who worked as civil servants has a better knowledge score in records with a mean percentage enhancement from 45% in the preintervention to 88% in the post intervention. The plausible explanation for this is that many working-class women in the Gambia often attend clinics in private facilities or special clinic days in public facilities where they had the opportunities to interact and obtained adequate health information from service providers. Therefore, this working-class women’s interaction with service providers in special clinic days coupled with this study’s educational intervention potentially produced a synergistic effect on their knowledge of breast cancer.
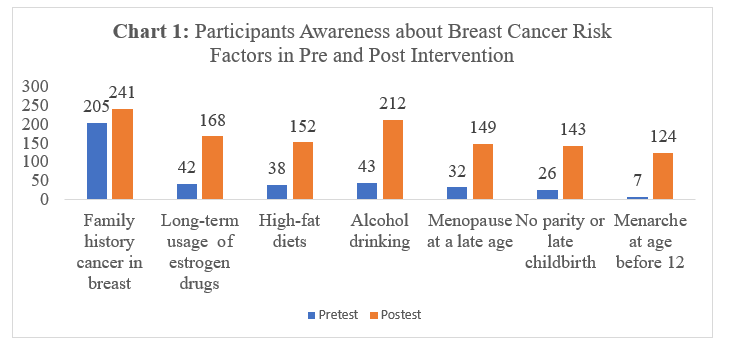
Consistently, this study showed an increase mean score in the participants awareness on the risk factors of breast cancer from the pre-intervention data collection to post-intervention data collection. Overall, post-intervention data shows that many participants highlighted family history and alcohol drinking as highest risk factors responsible for increase in breast cancer. Many Gambians do understand that diseases are related to “blood” which in the scientific context means the genetic/family history. The largest increase was the number who cited alcohol as the highest risk factor from 43 responses in the pre-intervention data collection to 212 responses in the post-intervention data collection with a difference of 169 responses. A Muslim-dominated country, where alcohol consumption is shunned, it is easy to convince not only the study participants, so also the general population, about the negative associations between alcohol and non-communicable diseases. Therefore, this post-intervention increases in knowledge score regarding alcohol consumption and the increased risk of breast cancer is not very surprising. However, this findings are in agreement with those from the Eastern China studies were family history of breast cancer was the best accepted risk factor for breast cancer among participants (18). Although there was a general post-intervention improvement in the participants’ knowledge on the risk factors for breast cancer, less that 50% of them agreed that menopause at late age, no parity or late childbirth and menarche at age before 12 increases the risk of breast cancer.
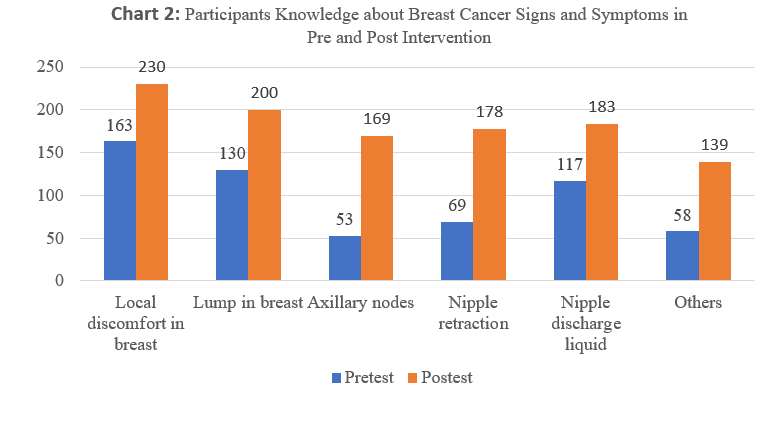
The post-intervention data analysis showed an increase in participants knowledge on breast cancer sign and symptoms, a finding in consonance with a community-based study held in Mumbai, India, in which between 56% and 75% of the participants indicated lump in breast, change in shape and size of breast, lump under armpit, and pain in one breast as important and common symptoms (12).
The multiple logistic regression results showed that knowledge and awareness level of breast cancer was associated with participants’ age, educational level, occupation, and household income. Women aged 35 to 40 were more likely to have a good knowledge about breast cancer compared to the reference category aged 25 to 34 [AOR: 0.303, 95% CI: (0.142–0.648)]. Women who obtained college level education has an odd of [AOR: 0.209, 95% CI: (0.049–0.890) compared to those with primary level education. Monthly household income also influences the knowledge level in the post intervention study and household income between D10,000 and D20,000 were [AOR: 0.335, 95% CI: (0.177–0.631)] and household income of over D20,000 where [AOR: 0.192, 95% CI: (0.074-0.500)] compared to those whose household income was less than D10,000. This is similar to a study conducted in China where a multivariate analysis (α = 0.05) identified age, location, occupation, family history of breast cancer, household annual income, behavioral prevention score, smoking and drinking habits, and overall life satisfaction to independently correlate with breast cancer awareness in China.(18)
Women aged 35 to 44 have the highest enhancement of knowledge with a mean increase from 24% in the pretest to 73% in the post test. The higher a woman educational level is the more their knowledge and awareness level increases after the intervention. This could be related to the following reasons: many of those who have obtained college level education and above falls within this age category and are more likely to be informed consequent of the effect of education, access to information and possible improve socioeconomic status. This could be associated to their literacy competency and the ability to read and make individual research about issues once introduced to them unlike their counterparts who mainly relies on their ears for such opportunities. Obtaining a college level education shows a good knowledge in both pre and post intervention. This shows that higher education is significantly related to breast cancer awareness and knowledge which could be related to both the type of training and the literacy level. Highly educated women are more likely to read journals, magazines and follow news than low educated women in the Gambia. In a study that assess knowledge of breast cancer and sources of information among women in Riyadh were 84% were Saudi national and 67.8% had a university level education. Eighty percent were between the ages of 20 to 50 years. The Knowledge of breast self-examination (BSE) was found to be high; 82% (95% confidence intervals [CI], 79.2–84.4%) (20). Increase in breast health awareness help to educate women about the importance of diagnosing cancer at early stages when treatment is easier, and outcome is better. Advanced cancers demand more extensive therapies and are more likely to metastasize to other organs at which point they no longer can be cured (21).
As participants house income increases so as their knowledge in both pre and post intervention. This could be associated with the fact that those whose earnings are more are predominantly youths, well-educated or those involved in lucrative business that provide them the opportunity to benefit from quality health services and information regardless of their geography. Findings from an Indian study concluded that cancer prevention policies should focus on leveraging the positive effects of better socioeconomic status, employment, health insurance ownership, exposure to electronic media, and better healthcare autonomy because it was found that higher age, urban residence, higher education, having employment, health insurance, use of electronic media, higher household wealth quintile, having healthcare autonomy, showed a positive effect on taking screening services due to increase awareness and knowledge (22).
The hypothesis on the effectiveness of health education intervention among participants which was tested using a paired sample T-test shows a significance difference in the pre intervention and post intervention awareness and knowledge. Improvements in all the various dimensions of the participants’ knowledge on breast cancer leading to the rejection of the research’s null hypothesis, and the acceptance of the alternative. The study’s findings agree to a great extend with a recently published study conducted in India, which concluded that community-based educational interventions were effective in enhancing knowledge regarding breast cancer among women(23).
It is not surprising that many participants cited a lack of information on the awareness about breast cancer because many participants claimed that this research was their first time to participate and adequately interact with health personnel on breast cancer-related programmes. Other perceived barriers to awareness include cultural beliefs and stigma about breast cancer. Sticking to cultural believes on serious health challenges such as breast cancer-related matters could be reduced by working with local authorities and training local women representative to bridge the gap that hinders access to healthcare through culturally acceptable programmes. This though is corroborated by Bhatt and Bathija (2018) that communities encompass a mix population from both low-and-high income individuals that face multifaceted challenges in accessing quality healthcare, which include; limited educational opportunities for some, reduced access to healthcare facilities, cultural barriers, and a lack of health education and awareness intervention(24).
An Ethiopian study on cervical cancer screening uptake study at selected health centres in Addis Ababa concluded that providing focused health education supported by printed educational materials increased the uptake of cervical cancer screening services by 74%(17) The current Gambian study found that the most preferred choice of health education or communication approach by women was the use of pamphlets or brochures and making videos or multimedia presentation in the peri-urban settings, a consequence of the socio-economic context of the area and the previous use of these mediums in health promotion and education programs and interventions. Uptake of maternal and child health services is promising in the Gambia. Therefore, providing a take-home educational material into the existing maternal and child health services can help increase cervical cancer awareness and screening uptake. The formal way of addressing health challenges among women Gambian is through organizing workshops or community-based activities that promotes women involvement in dialogue and education. These enable women in white-coloured jobs take official permission for participation and foster dialogue and participation among the different actors of the women’s health.
The limitation of this research is its inability to explore the relationship between proximity to health facilities and community demographics that affect participants’ knowledge on breast cancer.

{kind=link}
{kind=link}