Primary congenital lymphedema (PCL), also called Milroy disease (OMIM:#153100, MD) is caused by developmental lymphatic vascular anomalies, with an estimated prevalence of 1 in 160,000 individuals[17]. We reviewed the reported phenotypes of the Milroy disease, (Table S9. Review of clinical phenotypes of Milroy disease) that MD patients usually exhibit lymphedema at birth with swelling of the lower-limb, and most are bilateral[2]. They often have brawny texture and hyperkeratosis of foot skin; (Table S9: Review of clinical phenotypes of Milroy disease). The other phenotypes associated with MD including: Hydrocoele of male (37%), “ski jump” toenails (14%) and bilateral pleural effusion[2] (Table S9: Review of clinical phenotypes of Milroy disease). Although below knees lymphedema is the most common phenotypes of MD, edema of some patients extends to thighs [2, 18]. Meanwhile, hydrocoele is more common in male patients [2, 3, 19–22].
The FLT4 (FMS-LIKE TYROSINE KINASE 4; FLT4; NM_182925.4) gene mutations cause kinase-inactivation and Milroy disease [6, 7, 22–27]. to date, all mutations located in either of two intracellular kinase domains [6, 7]. In this research, we sequenced the tyrosine kinase coding domains of FLT4 gene in a large hereditary congenital lymphedema family which presents Milroy disease phenotypes, and found a missence mutation of c.T2774A which leads to the Valine to Glutamic acid substitution exchange (Fig. 4 Sanger sequencing result of the FLT4 gene c.2774 T-A mutation. p.V925E). This missence mutation causes the major phenotypes of Milroy disease in our pedigree members.
Interestingly, two patients suffered for specific clinical phenotypes compared with other patients within the family: patients I1 complaint that edema of his bi-legs aggravated and extend to the roots of the thighs when he caught cold and fever from childhood; Meanwhile, patient II1 complained that: as for childhood, edema continued to the lower extremities beneath the knees, and lymph fluid caused thinning and deforming of skin tissue, combined with proliferation of adipose and connective tissue, lead to swelling and bulky of feet. The lymphedema phenotype is not visible now due to plastic surgery, but the heavier lower extremities edema and “elephant-like” skin hyperkeratosis appearance of her legs is obvious (Fig. 2 − 1,2: bilateral lower limbs lymphedema of patient II1) [4, 28, 29]. On the contrary, the phenotypes of the other patients (except I1 and II1) are not like these two patients: lighter below knees lymphedema could be found in most of the patients within our family (Fig. 2–3: bilateral lower limbs lymphedema of patient II6; Fig. 2–4: bilateral lower limbs lymphedema of patient III3), some of the patients’ lymphedema is hard to see (II2, II4 and III4), neither the brawny texture of the skin; No hydrocoele has found within the male members.
As for now, reporters believed that the major pathologic changes of Milroy disease are aplastic, hypoplastic and dysfunctional cutaneous lymphatic vessels [6, 12], which fail to transport the fluid into the venous circulation, result in a lymphatic fluid stasis and swelling of the extremities [30–33] That is, lymphatic vessels malformation triggers the increase of interstitial protein rich fluid, results in insufficient lymphatic drainage and transport [34]. As a result, large amount of protein-rich fluid accumulates in tissue interstitial spaces, makes skin, subcutaneous tissue, fibrous tissues hyperplasia, and oppress of lymphatics more difficult to reflux for lymphatic; the edematous fluid and adipose tissue accumulate subcutaneously, and followed by inflammatory response developing and forming a vicious cycle that aggravating the formation of edema [19, 35]. Meanwhile, slowed down of lymphatic flow incites lipogenesis and fat deposition and leads to increased fibrocyte activation and connective tissue overgrowth [36–38]. Firmer subcutaneous tissue as fibrosis, hypertrophy of adipose tissue presents, these pathologic changes manifest initially as swelling of the affected limb or region, described as soft and pitting, but later progress to a more indurated state. The skin thickened, hardened, getting rough and bulky, and forming “elephant skin” swelling over time.
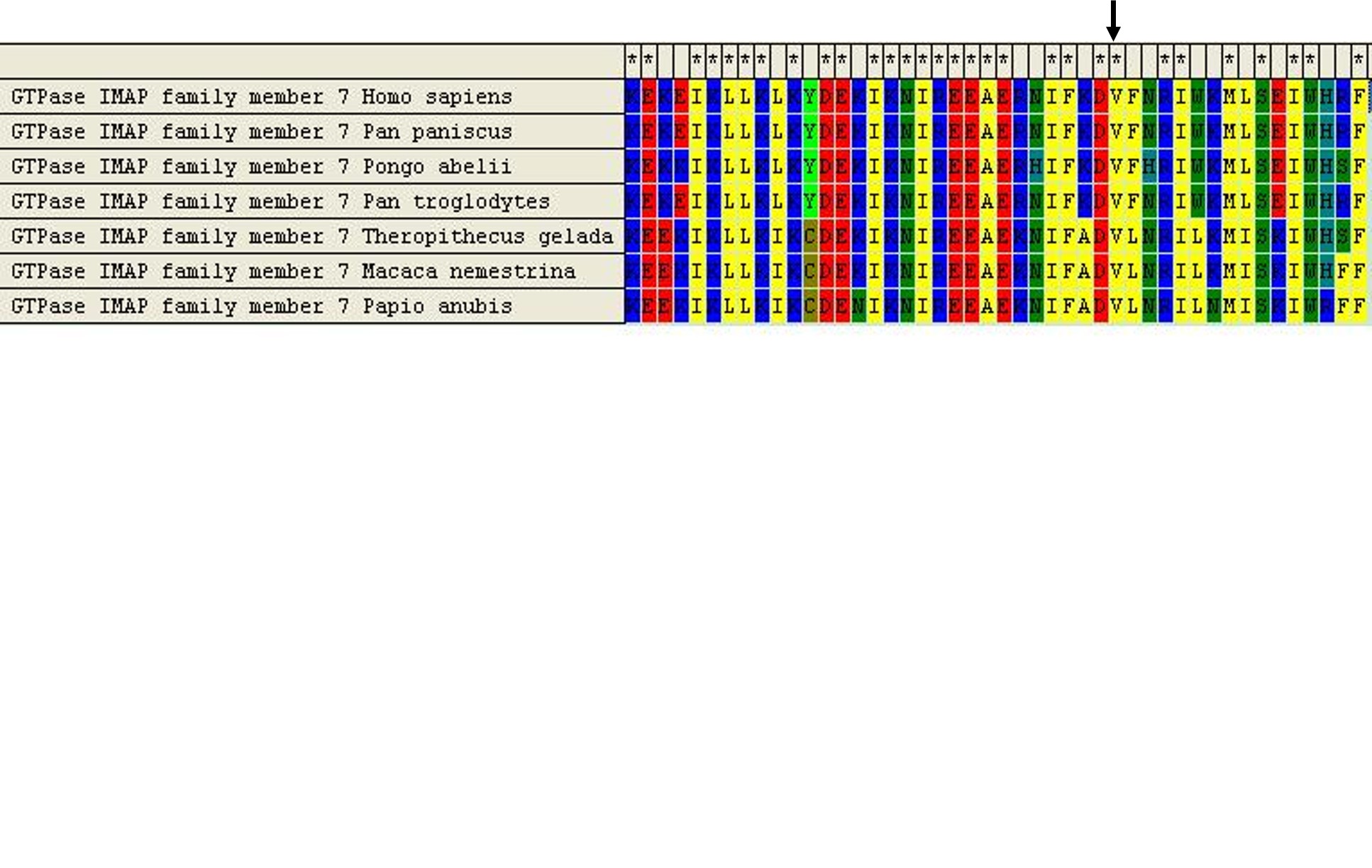
In our pedigree, we found two elder patients suffered for fever-related edema (I1) and heavier lower extremities edema and “elephant-like” skin hyperkeratosis appearance (II1), but phenotypes of other patients are not like them. The Heterogeneities of symptoms drove us to conduct NGS analysis to explore possible variants might be related to the phenotypes. Then we found a G deletion (c.826delG, p.Val276Phefs*29) of GIMAP7 gene in all patients except two (I1 and II1), neither in all the healthy controls. To date, there have been very few reports on the gene function of GIMAP7 gene. GIMAP7 gene belongs to the GTPase family, which is a family of immuno-related proteins (GIMAPs, GTPase of immunity-associated proteins), is widely expressed in the immune system and is differentially regulated during early human Th-cell differentiation[39]. The GIMAPs have been closely linked with cell survival of lymphoid cells[40]. Regulation of cell viability of death is likely to be regulated through GIMAP family members in immune cells. And the expression of GIMAP7 gene in normal tissues is higher than that in tumor tissues and may play a regulatory role in the immune response regulation in coordination with other molecules[41]. We speculated that the G deletion (c.826delG, p.Val276Phefs*29) of GIMAP7 gene caused the malfunction and its coordination with other molecules, and finally jeopardized immune response of the body, then the patients in this MD family both showed different symptoms compared to the patients I1 and II1: eg. The immune related— such as cold and fever related edema, and serious “elephant skin appearance” of foot skin even the hyperplasia of foot tissue. On the contrary, in Milroy disease patients—— just like the patients I1 and II1 and other reported MD patients—— protein-rich fluid accumulates in tissue interstitial spaces and followed by inflammatory response developing–forming a vicious cycle that aggravate the formation of edema and hyperplasia, leads to “hyperkeratosis appearance” of foot skin[19, 35] and below knees edema. According to the PPI network, the FLT4 and GIMAP7 protein is not directly related, and several proteins were involved in the protein-protein interaction network (Fig. 6 Protien-Protein interaction network of GIMAP7 and FLT4 gene). And some of the involved gene function is immune-related. Eg. the LILRB2 gene. So we speculated that immune associated gene malfunction and protein interactions might be the main reason for the phenotype heterogeneities. Based on our findings, our genetics and research team suggested that: Further research on GIMAP7 gene function should be conducted to testify our hypothesis. Two mutations occurred within one family and orchestrated together to present phenotype differences is a new perspective to explore heterogeneities, and need further research and attention. GIMAP7 gene mutation can be used as a potential molecular target for future exploration.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}