Setting
The Balgrist University Hospital (incorporating the University Spine Center Zürich) is a tertiary referral center for SI and affiliated to the University of Zurich, Switzerland. Regarding SIs, it has a multi-disciplinary team composed of five spine surgeons (both Orthopedic- and Neurosurgery), three internist physicians, a hospital pharmacist, specialized wound nurses, musculoskeletal expert radiologists, three specialized nutritionist nurses, two to four dedicated physiotherapists, and up to four Infectious Diseases physicians who are specialized in orthopedic infections. Moreover, this team is supported by a research campus (Balgrist Campus) with BioBanking facilities and a Unit for Clinical and Applied Research with nine study nurses and two personnel with experience in biostatistics and investigational designs (www.balgrist.ch). Our study starts at the Balgrist, but is expandable to other national or international centers with experience in the treatment of SIs.
Study Objectives
We plan a prospective-randomized study of spine infections, for which the intraoperative debridement is part of the therapy. The primary study objective is to evaluate if 6 weeks of systemic and targeted antibiotic therapy postoperatively is not inferior to 12 weeks (non-inferiority trial) in case of infected in spinal implant-associated infections spine implants left in place. For spine infections without implants, this objective is the evaluation if 3 weeks of antibiotic therapy is not inferior to 6 weeks in postoperative spinal infections without an implant. The switch from intravenous to oral medication will occur early, in absence of sepsis sensu strictu, bacteremia or intestinal problems, at latest after one week of treatment. Secondary objectives are the assessments of differences in total costs, sick leave, adverse events, mechanical sequelae, handicap at 6- and 12-months post-treatment and the changes in the nutritional status during therapy. A third objective is the assertion of infected tissue/bone for future studies.
Finally, our study includes BioBanking and the evaluation of the nutritional status of the patient at the beginning and the end of SI treatment. Instead of throwing away, we’ll collect intraoperative tissue and/or vertebral bone for ulterior studies. Of note, BioBanking and participation in the clinical trial are exclusive among each other. Patients refusing to provide intraoperative tissue for BioBanking still have the choice to participate in the randomized study and vice versa.
Definitions and eligibility criteria for participants
SI is defined as having ≥ 2 local manifestations of inflammation (swelling or induration, erythema, local tenderness or pain, local warmth, purulent discharge); together with the same pathogen(s) retrieved in the microbiological culture of at least two intraoperative samples in antibiotic-naive cases. Systemic inflammation (fever, shivering, bacteraemia, hemodynamic alterations) or histological confirmations are facultative. Remission is defined as the absence of any clinical, anamnestic, radiological or laboratory signs of former (or new) SI within 12 months of follow-up. A diagnostic control puncture for the microbiological exclusion of dormant bacteria is not necessary. Of note, internal closed fractures and residual back pain can be interpreted as remission as long they are no signs of infection as defined. Figure 1 resumes the inclusion/exclusion criteria, Figure 2 the study flowchart.
Interventions and study conduct
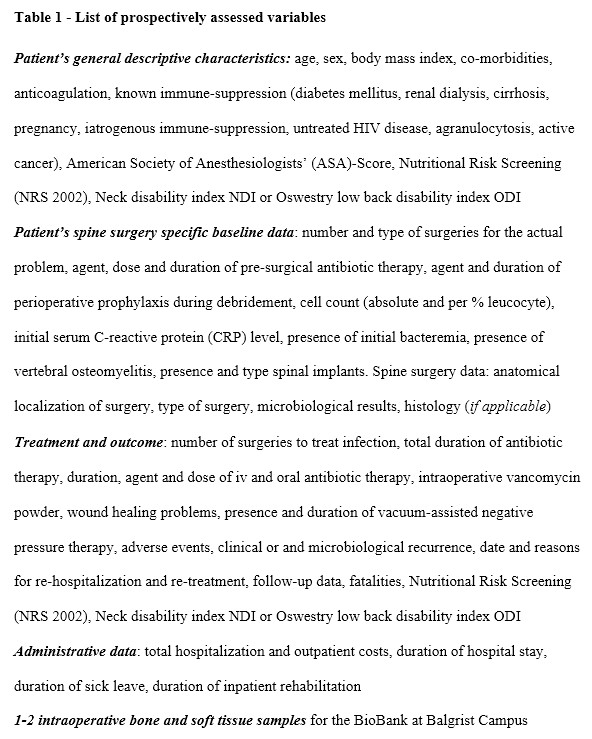
Upon individual consent of the patient, we will collect clinical, radiological, nutritional and laboratory data from each SI episode. The BioBank will store intraoperative specimens in the Balgrist Campus for 10 years. Table 1 reveals the variables of interest that we collect in the trials. The two RCTs depend on the presence of absence of infected osteosynthesis material:
- Infected spine material that was not entirely removed (or new material inserted):
Randomization between 6 and 12 weeks (+/- 4 days) of total antibiotic therapy counted since the first debridement for infection. Early switch to oral targeted therapy.
- Infected spine without residual material:
Randomization between 3 and 6 weeks (+/- 4 days) of total antibiotic therapy counted since the first debridement for infection. Early switch to oral targeted therapy.
After randomization, the study participants will be actively followed- up for 12 months. At database closure, we will review the medical charts of all patients to seek for unscheduled visits since the inclusion. This “passive follow-up” can reach up to four years and terminates at the date of database closure. The scheduled study visits take place as follows: visit 1 - Enrollment (Day 1), visit 2 - Day 15 (+/- 5 days), visit 3 - Day 21 (+/- 5 days), visit 4 - Day 42 (+/- 5 days), visit 5 - Day 84 (+/- 5 days). End of treatment visit 6 - Day 21, 42 or Day 84 (+/- 5 days) (only if still receiving treatment after visit 4). Test-of-cure visit - approximately (+/- 60 days) at 12 months (visit 7). The SPIRIT-Figure 3 resumes the timely assessments that are identical for both RCT.
Antibiotic agents
The antibiotic therapy is prescribed by Infectious Diseases physicians with experience in orthopaedic infections, the surgeons in charge of the patient, and/or the internists. It is administered by nurses experienced in orthopaedic infections. Initially, antibiotic therapy is either empiric or targeted to the results of preoperative bone biopsy. After 2-5 days, antibiotic therapy becomes targeted to the pathogens identified in microbiological cultures, and their antibiotic susceptibility profile. The choice of the agent, its intravenous or oral administration route, is usually at the discretion of the Infectious Diseases physician. However, for this study, and in order to achieve a minimal homogeneity, we established a list of “allowed antibiotics” and their recommended doses (Table 2). The investigators must choose among them, unless the causing pathogen of the spine infection is not listed in Table 1 or if an additional surgical site infection (e.g. postoperative pneumonia) needs a broad-spectrum antibiotic treatment. Of note, in this study, we will not test special doses or new indications for antibiotic therapy. Only the duration of the therapy will be determined. All antibiotics are already on the Swiss market and approved by Swissmedic, the corresponding authority for medication use. We avoid placebos, topical antibiotics and topical antiseptics; except for the pre-incisional skin preparation and (potential) use. Anaesthesiologists and surgeons are also free to comply with the prevention protocols, even if the patient is already infected, by administering the standard antibiotic prophylaxis (cefuroxime, vancomycin, or clindamycin) for up to three consecutive doses.
Pregnancy and breast-feeding
This cohort, all antibiotics and surgeries, have no specific relations to pregnant or breast-feeding women and their children. Additionally, the study population is likely not to reveal women at procreating age. Thus, pregnant and breast-feeding women are not excluded. The investigators will avoid agents that are not liberated for pregnant or breast-feeding women, according to the Swiss Compendium (www.compendium.ch).
Outcomes of interest
For the RCTs and BioBanking, we will collect data and biological material. Concerning the randomized trails, Table 1 (bottom) summarizes the outcome parameters. Regarding the investigation of the dynamic changes of the nutritional status during SI care, specialist nutrition nurses will assess the status at baseline and the end of treatment. In case of severe malnutrition, they are allowed to propose corrective measures already during the SI therapy, because it would be unethical not to intervene only because of study purposes. Finally, the database will be sufficient large to estimate the influence of an underlying chronic immune-suppression (i.e. diabetes mellitus, chronic steroid therapy, dialysis, untreated HIV disease, active cancer in therapeutic or palliative treatment, cirrhosis CHILD C) on SI outcomes and related nutritional status. We also reminder that patients with very severe iatrogenic immune suppression, such as recent solid organ or bone transplantations in the last five years, are exempted from the SASI trials (Figure 1).
Allocation and timetable
After written informed consent will been given to participants (until Day 5 of debridement), the unblinded allocation occurs electronically with a randomization scheme of 1:1 (randomization without blocked or matched variables). The study nurse of the Unit for Clinical and Applied research and/or the co-investigators will implement the allocation sequence into the trial. For both RCTs, we need 36 months of study time; starting in August 2019. Table 3 highlights some key time events.
Statistical analyses and sample size
Both RCT are non-inferiority trials. Remission incidence (at the first attempt of therapy) is set at 5% (5% recurrence in both arms). The clinically maximum acceptable difference (unidirectional non-inferiority margin with binary-outcome categorical variables) is arbitrarily fixed at 10% regarding the primary outcome remission [1]. Assuming a risk of alpha at 0.05 and a power of 80%, it will be necessary to recruit 59 patients in each antibiotic duration arm (short or long). Together with the distinction of the RCT into implant-related and implant-free SI, we would finally need 2 x 2 x 59 episodes, equalling a total of 236 SI episodes within three years. For assessment the formal non-inferiority requirement (regarding the primary outcome “remission”), we will compute with a unidirectional p-value limit of 0.025. We do not predefine a non-inferiority margin for secondary outcomes such as costs, adverse events, functional outcomes, underlying immune suppression, dynamic changes in the nutrition status and BioBanking.
Interim analyses
When the first 20 episodes of any randomization branch will have a complete follow-up, and again 60 and 120 SI episodes, we perform three interim analyses. On this occasion, we equally check if the expected statistical power for the final analysis will be acceptable. If it is lower than 30%, we will consider the trial will not be able to demonstrate the result, and the recruitment is no more ethical. The most frequent conditional power evaluated under the current trend (i.e. using the information from the collected data) will be assessed [7,8]. The Study Data Monitoring Committee will consist of independent surgeons or physicians, with clinical and statistical experience, not participating in the study. They will decide about the future of the trial, entirely or partially, after each of the three interim analyses. The PI and the Sponsor will present the data in a blinded form to the Data Monitoring Committee. Their members will only know if there is an implant, but ignore allocations to the antibiotic arms.
The intent-to-treat (ITT) population will consist of all randomized patients who signed for the participation. Patients will be analysed according to treatment group assignment regardless of whether the patient receives any treatment or the wrong treatment or is lost to follow-up. The per-protocol (PP) population will consist of all patients who complete the study and who have not deviated significantly from the protocol. The statistical analyses will mostly base on descriptive analyses, group comparisons and a multivariate, unmatched, eventually cluster-controlled, Cox regression analysis adjusting for the large case-mix that we expect. Equally, a Generalized Estimation Equations (GEE) model might adjust for clustering in case of multicentre origin of the patients. The Biostatistician will analyze the datasets in a blinded form (as group A or B), but the PI, the Study Nurses, and the Sponsor will ultimately unblind the allocations for data verification and definition of the ITT and PP populations.
Ethical and regulatory aspects
Study registration, ethical conduct and categorization
The study is approved by the Ethical Committee of Zurich (no. 2019-00646) and registered in the Swiss Federal Complementary Database („Portal“) and in the international trial registry ClinicalTrials.gov (clinicaltrials.gov; no. NCT04048304). This study only makes use of the medicinal products and antibiotic agents that are already authorized in Switzerland. The indication and the dosage are used in accordance with the prescribing information and the international guidelines making this study fall into the category of Clinical Trials A. The study will be carried out in accordance to the protocol and with principles enunciated in the Helsinki Declaration, the Good Clinical Practice guidelines and the Swiss Law. The Ethical Committee receives annual safety reports and is informed about the study stop/end. Substantial amendments are only implemented after a new Ethical Committee approval.
Patient Information and Informed Consent
Participants will be recruited by any of the investigators of the study. Our institution has a standardized procedure for recruiting participants as participant studies are common. Each participant will be informed that the participation in the study is completely voluntary and that he/she may withdraw from the study at any time and that withdrawal of consent will not affect his/her medical assistance and treatment in the future. All participants of the study will be provided a Participant Information Sheet and Informed Consent Form entailing sufficient information. For the BioBank, the participants will sign the General Consent for the further use of personal data and biologic material. The investigators affirm and uphold the principle of the participant's right to privacy and that they shall comply with applicable privacy laws and/or the corresponding section of the study specific consent.
Safety issues
Monitoring
The Unit for Clinical and Applied Research of Balgrist University Hospital will assign an independent monitor. Regular monitoring visits at the investigator’s site prior to the start and twice during the course of the study will help to follow up the progress, to assure utmost accuracy of the data and to detect possible errors at an early time point. The monitor will review all or a part of the Case Report Forms (CRF) and written informed consents. The accuracy of the data will be verified by reviewing the above referenced documents. There will be a close-out visit at the study end. During the monitoring, all documents including source data/documents will be accessible for the monitor.
Audits and Inspections
An audit/inspection of this study may be conducted by the competent authority. The quality assurance auditor/inspector could have access to all medical records, the investigator's study related files and correspondence, and the informed consent documentation that is relevant to this clinical study. The investigator will allow the persons being responsible for the audit or the inspection to have access to the source data/ documents and to answer any questions arising. All involved parties will keep the patient data strictly confidential.
Early termination of the study (participation)
The investigators may terminate the study prematurely according to certain circumstances, for example: ethical concerns, insufficient participant recruitment, when the safety of the participants is doubtful or at risk, respectively, alterations in accepted clinical practice that make the continuation of a clinical trial unwise, early evidence of benefit or harm of the experimental intervention. If a patient is withdrawn, the reason will be noted. When possible, evaluations required at the next scheduled visit will be performed at early termination.
Treatment by specialists
All surgeries will be performed in the supervision and participation of an experienced spine surgeon. The antibiotic therapy is ordered and supervised by internists and infectious diseases physicians with therapeutic and academic experience in SI treatments. The current medications of the study patients, as well as possible interactions, will be controlled by the internists several times a week during hospitalization.
Definition and assessment of (serious) adverse events and other safety related events
An Adverse Event (AE) is any untoward medical occurrence in a patient, and which does not necessarily have a causal relationship with the study procedure. A Serious Adverse Event (SAE) is classified as any untoward medical occurrence that: results in death, is life-threatening, requires in-patient hospitalization or prolongation of existing hospitalization, results in persistent or significant disability/incapacity. In addition, important medical events that may not be immediately life-threatening or result in death, but may jeopardize the patient or may require intervention to prevent one of the other outcomes listed above should also usually be considered serious. Participants with ongoing SAEs at study termination will be further followed up until recovery or until stabilization of the disease after termination. The investigators will make a causality assessment of the event to the study. All SAEs must be reported immediately and within a maximum of 24 hours to the Sponsor-Investigator of the study. SAEs resulting in death are reported to the local Ethics Committee (via local Investigator) within 7 days. Patients with adverse events, and leaving the study, will be treated off-study, without restriction, at the study site.
Case Report Forms, procedure of data analysis and BioBank archiving
An electronic CRF will be generated for every patient. All relevant study data are recorded by authorized persons in the REDCap® electronic data capture tool [9] and archived for a minimum of 10 years. Participating patients will be registered in an enrolment log assigning the participant to his/her study ID. Corrections can only be made by the authorized persons. For data analysis, subject-related data from REDCap will be exported and analyzed in statistics software (IBM - SPSS and/or STATA). Before data export, all patient identifiers will be removed. Patient-source and BioBank data will be registered using subject identifiers. Collection, disclosure, storage of patient-related data is carried out in accordance with Swiss data protection regulations and the Human Research Act. The BioBank will store the intraoperative tissue samples in accordance with their guidelines. Likewise, radiological data are stored in the PACS system according to the standard at the Balgrist University Hospital.
Theoretical risk of the study
Besides the retrospective identification of patients, we do not see any particular risk for the patients regarding the cohort. For BioBanking specifically; a theoretical additional risk could be the detection of unknown pathologies, if there would be a further work-up of the intraoperative samples. Concerning the RCTs, a theoretical risk could be a higher incidence of recurrences in the corresponding short antibiotic arms.
{kind=link}