Of the selected mothers, 1265 responded to the questionnaire, giving a response rate of 97.3%. Participation from individual wards ranged between 76.5% - 100%. Of the non-respondents, four did not consent for participation (0.3%) and another 31 mothers (2.4%) who consented, had left the hospital before the interview was initiated.
The inter-rater reliability was satisfactory for all the data collectors as all had obtained an Intra class correlation coefficient between 0.96–0.99.
Socio demographic and pregnancy related details of the participants
Age ranged from 16 to 46 years, while most mothers belonged to the 20–35 years age group (n = 1074, 84.9%). More than three fourths have obtained an educational qualification above the secondary level (n = 1029, 81.3%). A clear majority of the study sample (n = 958, 75.7%) was unemployed. Average monthly income showed a wide variation, ranging from Rs.3,000.00 (17 USD) to Rs.350,000.00 (2000 USD). Close to half of the study sample were primi mothers (n = 525, 41.5%) (Table 1).
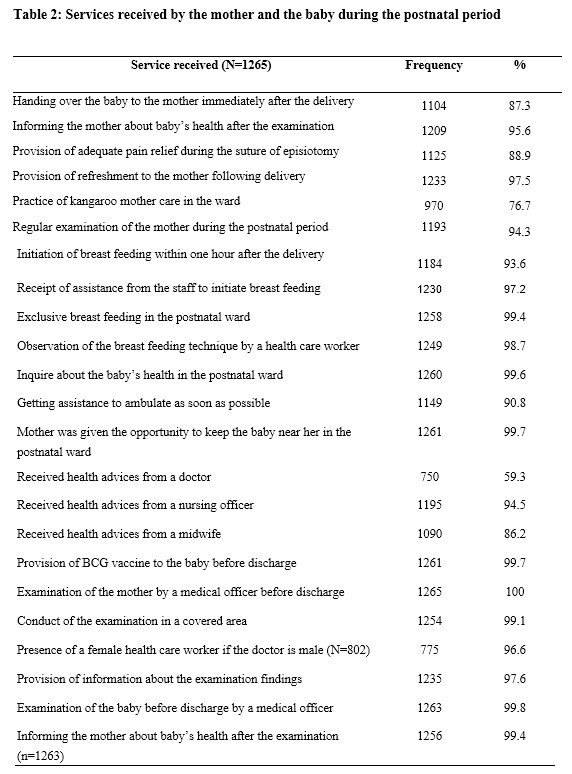
Mothers’ account on services received by them
Services recommended in the national guidelines to be delivered during the postnatal period following a NVD were received by most of the participants. Majority have initiated breast feeding within one hour after delivery (n = 1184, 93.6%) as recommended, and 99.4% mothers have exclusively breast fed while in the postnatal ward. The technique of breast feeding has been assessed by a health care worker for majority of mothers (n = 1249, 98.7%) and corrected where necessary. Least frequently received service was the opportunity to practice kangaroo mother care (KMC) (n = 970, 76.7%).
Inquiry was made into the services provided to the mother and the newborn at discharge. All the mothers and 99.8% (n = 1263) of the babies have been examined by a medical officer at discharge, and over 95% of the examinees were informed about their examination findings (1235 participants were informed about their examination findings and 1256 were given information following examination of the baby). Privacy has been ensured during 99% of the examinations by covering the examination area (n = 1254).
All mothers have received health advices regarding the postnatal period. The main sources of information were nursing officers and midwives (n = 1195, 94.5% and n = 190, 86.2% respectively). Medical officers have provided health advices to only 750 mothers in the study sample (59.3%) (Table 2).
Client perceived quality of institutional postnatal care (CQIPNC)
The total obtainable score of CQIPNC ranged from 23 to 115. The obtainable scores for technical care and information domain, interpersonal care domain and ward facilities and cleanliness domain ranged between 9–45, 7–35, and 7–35 respectively.
The total score obtained for the CQIPNC questionnaire in the study ranged from 48 to 115. The median score obtained was 108, which was 93.9% of the total obtainable score (IQR- 96–114). Technical care and information domain had a median score of 43 (IQR = 38–45). Interpersonal care domain and ward facilities and cleanliness domain had median scores of 33 (IQR = 30–35) and 32 (IQR = 28–35) respectively (Table 3).
Over 90% of the mothers have rated care as ‘good’ or ‘very good’ for all the items included in interpersonal care domain and the technical care and information domain. The ratings reduced somewhat for the items in the ward facilities and cleanliness domain. Only 81.1% have rated the cleanliness of the toilets in the ward as ‘good’ or ‘very good’. The ‘good’ or ‘very good’ ratings percentages for the space and the facilities available were 88.0% and 88.8% respectively (Table 4).
Determinants of client perceived quality of care
The bivariate analysis depicted that participant characteristics such as the age between 20–35 years (OR = 1.6, p = 0.06), husband’s occupation (OR = 1.2, p = 0.08), average monthly income (OR = 0.8, p = 0.13), the type of institution used by the mother (OR = 1.4, p = 0.004); services such as initiation of breast feeding within one hour (2.2, p = 0.001), informing the mother after examination of the baby (OR = 1.9, p = 0.02), provision of adequate pain relief during episiotomy suture (OR = 2.2, P<0.001), giving assistance to practice KMC in the labour room and the ward (OR = 1.4, p = 0.02), receiving health advices from doctors (OR = 2.6, p<0.001) and midwives (OR = 3.2, p<0.001), regular examination of the mother (OR = 2.0, p = 0.009), getting assistance to initiate breast feeding (OR = 1.9,p = 0.12) were significantly associated with high perceptions of quality of care.
Among these variables, only 20–35 age category (aOR = 1.8, p = 0.024), teaching and specialized hospitals category (1.6, p<0.001), and services such as initiation of breast feeding within one hour of delivery (2.1, p = 0.009), pain relief during suturing of the episiotomy (2.2, p<0.001), Ability to practice KMC (1.4, p = 0.035), Receiving health advices by the doctors (2.1, p<0.001) and PHMs (2.1, p<0.001) were identified as significant correlates via the multivariate analysis (Table 5).
The final model explains between 10.7% (Cox & Snell R square) to 14.3% (Negelkerke R Square) of the variation in the client perceived quality. The Omnibus test was statistically significant with a p value of less than 0.001. Hosmer and Lameshow test was not significant, indicating that the model was a good fit to the data. The final model of the binary logistic regression correctly classified 52.5% of client perceptions.
{kind=link}