The traditional method for the pre-surgical planning of hip replacements is a physical x-ray with a magnification between 10% and 20% [8, 9]. Two types of templates are used for planning: the acetabular cup and the femoral component. The profiles drawn on the transparent templates overlap the hip radiographs where the anatomical segments are found until the size that fits is found [17]. The accuracy has been reported of 52% in the acetabular component and 56% in the femoral component [22].
The emergence of new digital technologies has decreased the use of physical radiographs, altering the traditional way of pre-surgical planning for joint replacements [12, 22]. In the market, there are multiple software that allows digital planning however, their costs are high, especially in the context of a developing country. Available literature has reported an accuracy of 38% of the acetabular component and 35% of the femoral component using this method [23].
Hybrid planning was initially described in 2006 for total hip replacements, consisting of measuring digital images on a liquid crystal monitor to scale so that the image magnifier is the same size as the metric system of the templates used for planning. After this, traditional planning is carried out with acetates [24].
In 2015 Petretta et al. found an accuracy of 77% and 0.75 in the planning of the acetabular and femoral component respectively. In their study, 260 measurements were made by 5 different people with different levels of experience on radiographs of 52 patients. They found no inter or intra-observer differences and when compared against digital planning. Additionally, it was superior in the planning of the femoral component compared with the digital method, without differences in the acetabular cup [13]. Also Wang et al, in 2017 report ICC for acetabular templating of 0.918 and ICC for femoral component templating of 0.944 [25].
Taking into account the context of a university hospital in a developing country, we seek to save costs and at the same time achieve a reliable and highly effective method to obtain the best clinical results in our patients. The above motivates us to study the precision and accuracy of this method.
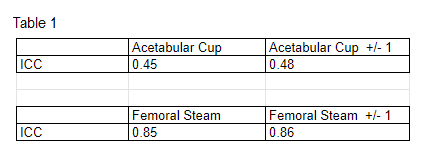
Our study shows that preparatory planning with the hybrid method has adequate accuracy when compared to the prosthesis that was finally implanted. The femoral component presented in all measurements a correlation near 0.9 (even without adjustment of sizes) which is interpreted as excellent [26]. Similarly, no differences were found concerning the level of experience or training of the person who made the measurements. This accuracy was so high that we may infer that in the clinical setting planning the femoral component could not require to take a size above or below.
On the other hand, the accuracy of the acetabular component was moderate in all measurements (around 0.45) [26]. However, in this case, having one size above or one below did not significantly affect the accuracy. A hypothesis that may explain the low reliability is that acetabulum is a tridimensional structure with ellipse shape, which hinders the measures more than a circumference structure, such as the femur diaphysis. Furthermore, if we take into account that plain radiography represents only two dimensions. Results suggest that in clinical practice the minimum need for one or two sizes above or below the planning should be anticipated before entering surgery.
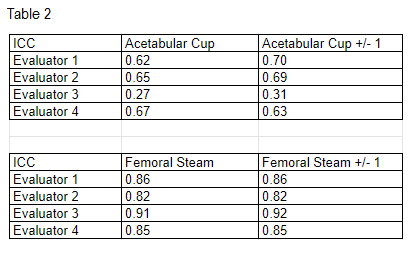
It is important to mention that when an independent analysis between the observers was made, significant differences were noticed (Table 2). This was especially important in the acetabular cup measurement of evaluator 3 which had very low ICC, even with the size correction the discrepancy in relation to the others was significant. When we performed a retrospective analysis, we found that this evaluator had had an error in the calibration of the measurements in a systematic way that could explain his inferior results.
{kind=link}
{kind=link}