Analytical Framework
This paper followed the conceptual framework proposed by Ronald. M. Anderson [16] to analyze the healthcare service access and utilization. According to this model, the population healthcare utilization behavior is determined by three factors: predisposing, enabling, and need. These factors can influence the healthcare utilization at both the individual and contextual level. The predisposing factors include demographic and socioeconomic characteristics of the individual, i.e., gender, age, marital status, place of residence, employment status, social class, attitude, and knowledge of healthcare services. The enabling factors comprise resources that directly or indirectly affect the ability to afford the healthcare services, for example, wealth or income, social security, health insurance etc. The need factors refer to the need to be perceived by ailing person or need to be gauged by a health professional. This study has some data-related limitations; for example, the data is not available on social class, attitudes and knowledge of the elderly, and types of ailment and treatment sought.
Therefore, our behavioral model includes selected predisposing and enabling factors for which the information was available. Further, the dataset did not provide information on the types of ailment, treatment, expenses on medication, rehabilitations, clinical tests, and duration of hospitalization. Therefore, we used the frequency of the consultation as one of the components of the factors of healthcare utilization. The following is a diagrammatic representation of the analytical framework used in the study (Figure 1). Several previous studies have modified the framework to accommodate the respective contexts of healthcare utilization behavior of the population [16, 17, 20–24].
Data Sources
This study used data from Pakistan Social and Living Standards Measurement (PSLM) Survey (2014-15), the largest administrative dataset sponsored by Pakistan Bureau of Statistics (PBS). The data set is representative at the national, provincial, and district level. The purpose of this survey was to collect information on health, education, assets, and economic condition of households, water, and sanitation, and the satisfaction of households by facilities and services used. PBS has developed its sampling frame for both urban and rural domains segregating each city/town into enumeration blocks, and each block consisted 200 to 250 households with specific boundaries and maps[10].
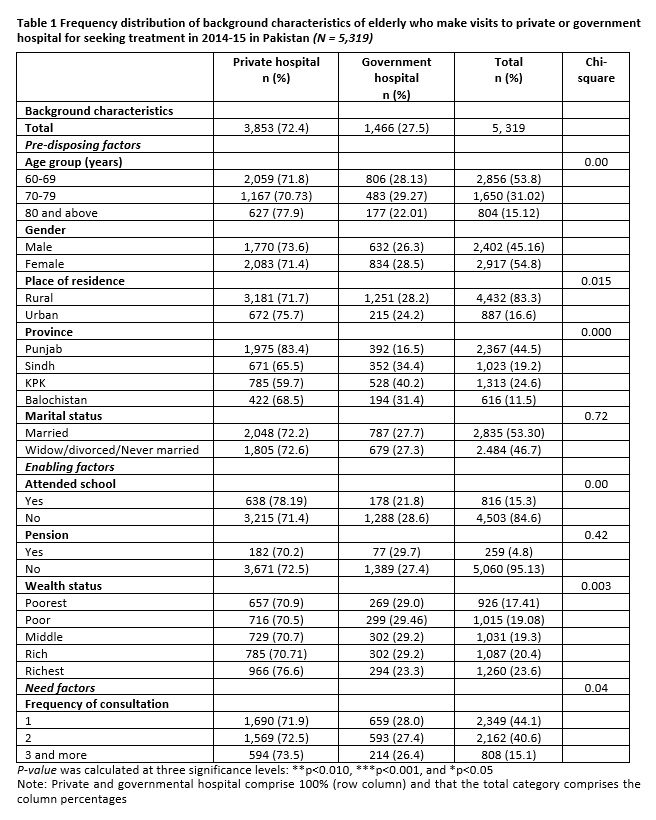
Given the survey’s objectives, the sample size for the four provinces has been fixed at 5,428 sample blocks comprising 81,992 households. This study limits elderly participants from 60 years and above. Given this limitation, a total of 5,319 participants were identified and examined for visiting private or government hospital to meet their healthcare needs. The selected sample represents retired personnel from formal sectors as well as working adults aged 60 and above in the informal sector. The data of behavioral factors, such as age, gender, marital status, region, province, education, wealth status, frequency of consultation and pension, of healthcare utilization was considered for empirical analyses.
Variable description
Healthcare Services
The study used information on the utilization of healthcare services collected from individuals aged 60 years and above. The information was available on whether the interviewed person fell sick in the past two weeks or not, and in case he or she fell sick, did she consult private or government or other healthcare provider for consultation. The “other consultation” included less than three percent of the overall responses.
The private hospital denotes visits to private dispensary/private hospital, and government hospital implies visits to government hospital/dispensary, rural health unit, basic health unit, and includes others as well. The section D—Health of the PSLM questionnaire and questions 1-3 were used to extract the required data and form a variable. We combined “other consultation” with the government. We used two outcome variables: private hospital visits and government hospital visits. Each outcome variable was measured as a binary response (1/0), where 1 refers to visit(s) s/consultation(s) to/at government hospital/private hospital, and 0 means no visit/no consultation.
Behavioral factors
The predisposing factors included gender, region, age groups, province, and marital status. The gender was measured as a categorical variable; male, and female. The place of residence was a categorical variable coded as rural and urban; age groups were categorized in years-group 60-69, 70-79, 80 and above; the province was classified as Punjab, Sindh, Khyber Pakhtunkhwa or KPK, and Balochistan. Marital status comprised two groups, married, and unmarried/widower or widow/ divorced.
The enabling factors were wealth status, pension and attended school. A better wealth status and availability of social security after retirement enhances the ability of the elderly to use healthcare services, and education helps to gain knowledge about the availability and quality of health care services. The different quintiles of the wealth status, a composite index of household asset, was assigned codes in ascending order, poorest, poor, middle, rich, richest. The availability of social security or pension after retirement was categorized as ye and no. Attended school was measured as a binary variable; attended; not-attended
Moreover, frequency of consultation was used as the component of the factors of utilization of outpatient services, and it was measured by asking the interviewee that how frequently he or she visited the hospital in the last two weeks’ prior the survey. The answers were recorded, as follows; only once, two-times, three times, and so on. We grouped all responses into three categories; once; two-times, three times and more.
Statistical analysis
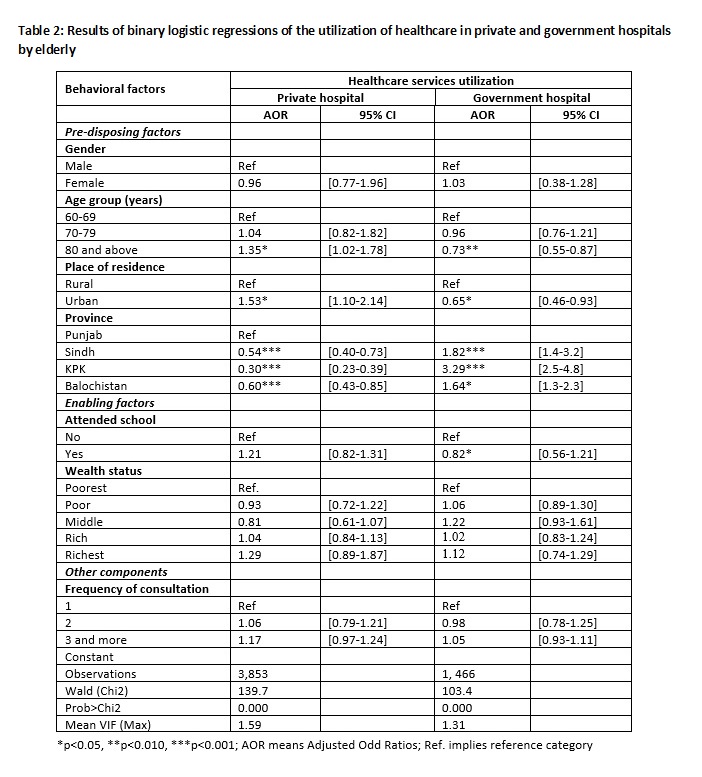
This study used univariate analysis to examine the background characteristics of the sample. The association between healthcare services and various behavioral factors was analyzed using Chi-square test. Subsequently, a binary logistic regression was used to examine the predicating factors of healthcare services utilization in private or government hospital by the elderly. The model is considered suitable when the dependent/outcome variable, such as the use of healthcare services in private or government hospital, is dichotomized or (0/1). The predicted value was described using adjusted odd ratios (estimated by taking the antilog of the logistic coefficient) at 95% confidence intervals [25]. The results were presented for three significance levels, P<0.05, P<0.010, and P<0.001.
It is pertinent to mention that the logistic model has some advantages over the simple linear probability model. The linear model states that probability is a linear function of the regressors, whereas the binary logistic model asserts that the natural log of the odds is a linear function of regressors. Unlike, the simple linear regression, a binary logistic regression can handle independent variables of any data level (binary, categorical, or ordinal). However, the logistic model is preferred to examine a series of independent variables that can best predict the outcome [26].