Study selection and quality assessment
We identified 18 potentially relevant studies[18–35] that satisfied the inclusion criteria, after the assessment for eligibility (see Fig. 1). There were totally 1769 patients in 18 studies with 899 patients in the experimental group and 870 patients in the control group, and all of them were included in the meta-analysis.
The antioxidant strategy and the mechanism of action are shown in Table 1. The characteristics of the included trials are summarized in Table 2. Stratified by the type of antioxidant strategy, in 2 studies[27, 28] albumin was used for treatment, 6 studies[20–23, 26, 31] used enteral feeding with antioxidants, 6 studies[24, 30, 32–35] used NAC for treatment, 1 study[19] employed selenium treatment, 1 study[18] was conducted with Vitamin C, 2 studies[25, 32] used Oxothiazolidine-4-carboxylic acid for treatment, and another study[29] used lisofylline for therapy. The mean age of the patients ranged from 42.4 to 72.5. The mortality of the control group ranged from 12.5–76.92%.
We evaluated the quality of the included trials according to the Cochrane’s risk of bias assessment table, and the results are shown in Table S1. As shown in Fig. 2 and Table S1, 2 studies[26, 30] were un-blinded, 3 studies[20, 22, 24] were singled-blinded, and 1 study[35] did not report on the blinding of participants and personnel and was considered as high risk or unclear. Nine of the included studies[20–22, 24, 25, 30, 33–35] were unclear about random sequence generation, as well as allocation concealment.
Effect on mortality
The random-effects model and fixed-effect model were both used to analyze the overall effect of each antioxidant therapy on mortality, and the results were coincident. As shown in Fig. 3, the results did not show any obvious reduction in the risk of mortality in ARDS patients treated with antioxidant therapies except vitamin C, a pool with only one study with 166 patients. The mortality of the included studies were between 0–53.13% in the treatment group, compared with 12.5–76.92% in the control group.
The mortality of the included studies varied between 5.9% and 55.6%. In view of the heterogeneity of mortality across the trials, we conducted a subgroup analysis by stratifying the meta-analyses according to the mortality of the patients in the control group. As shown in Fig. 4, the results revealed that there was a trend of gradual increased benefit with increased mortality. Furthermore, in ARDS patients with low risk of death, antioxidant therapies might be harmful (M–H RR, 1.52 (95% CI, 1.12–2.05); p = 0.73; six trials, n = 718), and should be avoided.
We also recorded the start time of the antioxidant therapy and conducted a subgroup analysis by stratifying the meta-analyses according to the start time. The results (as shown in Fig. 5) revealed that for a start time later than 24 hours, antioxidant therapy might be harmful (M–H RR, 1.37 (95% CI, 0.98–1.93); p = 0.29; three trials, n = 495). However, for trials that start within 24 hours, there was a trend of benefit from the antioxidant therapies, although the result was not significant (M–H RR, 0.73 (95% CI, 0.47–1.13); p = 0.10; four trials, n = 386). Therefore, in future trials the start time of the treatment is a factor that should not be ignored.
Sensitivity analyses
To test the robustness of the results, we conducted a sensitivity analyses by excluding individual study, re-analyzing, and comparing it with the original results. The results were consistent with the previous one.
Publication Bias
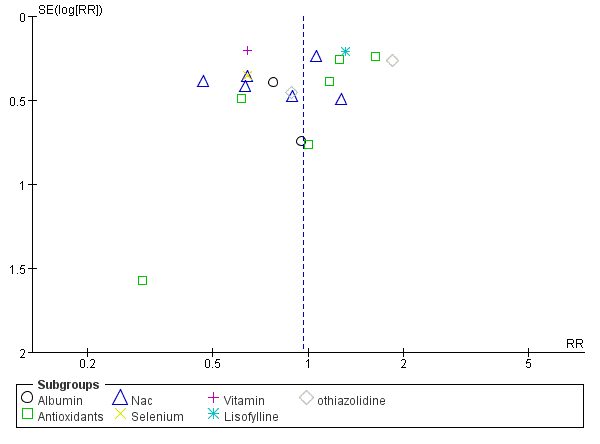
No evidence of publication bias was detected by the funnel plots (see Figure S1).
{kind=link}